
The Todani classification of bile duct cysts classically divides choledochal cysts into five groups.
On this page:
Classification
Traditional classification
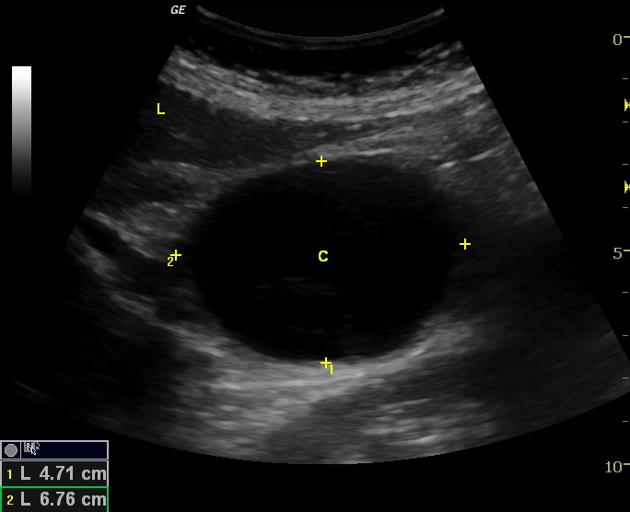
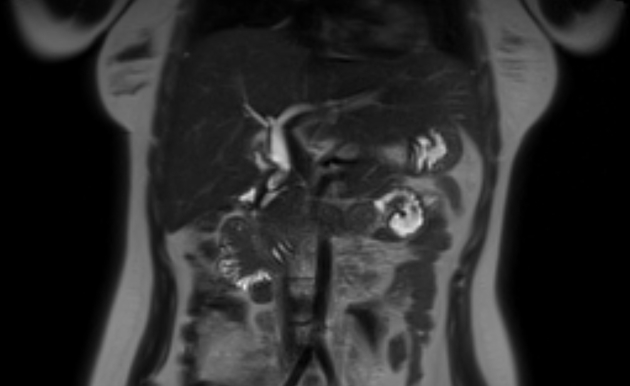
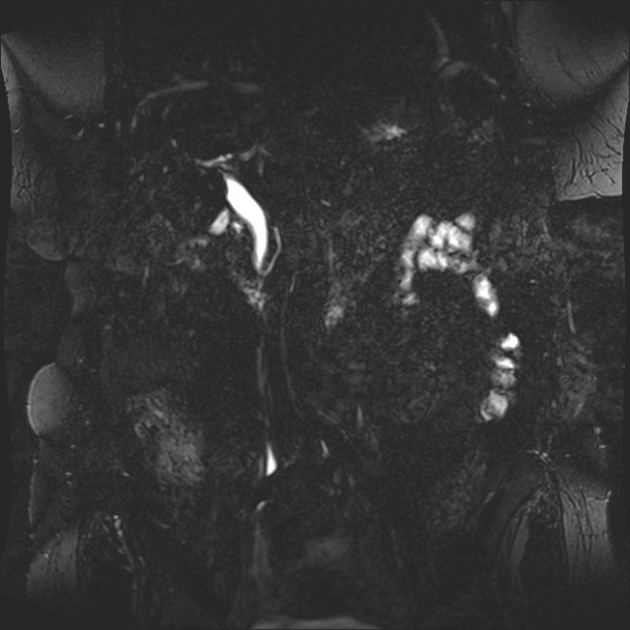
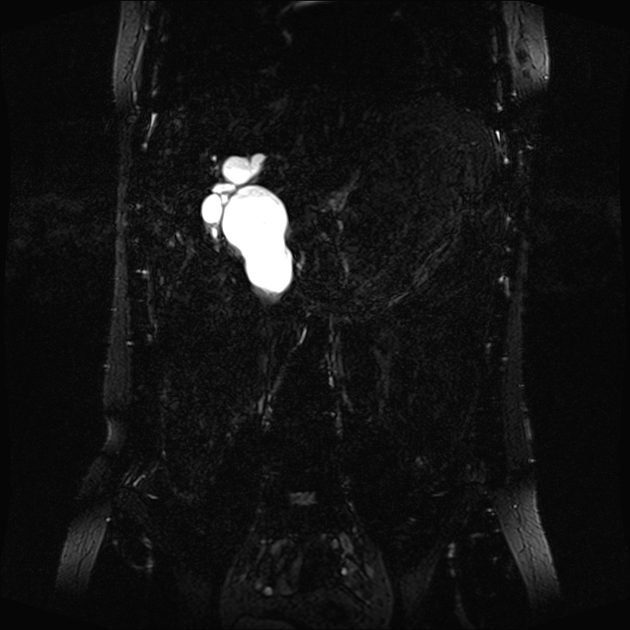
Type I
See: choledochal cyst - type I
account for 80-90% of all bile duct cysts
characterized by fusiform dilation of the extrahepatic bile duct
-
a subclassification has been proposed
Ia: dilatation of extrahepatic bile duct (entire)
Ib: dilatation of extrahepatic bile duct (focal segment)
Ic: dilatation of the common bile duct portion of extrahepatic bile duct
Theorized to form as the result of reflux of pancreatic secretions into the bile duct via an anomalous pancreaticobiliary junction. Some believe them to arise from ductal plate anomalies.
Type II
Also known as a bile duct diverticulum:
account for 3% of all bile duct cysts
saccular outpouchings, representing true diverticula, arise from the supraduodenal extrahepatic bile duct or the intrahepatic bile ducts
Type III
Also known as a choledochocele:
account for 5% of all bile duct cysts
represent protrusion of a focally dilated, intramural segment of the distal common bile duct into the duodenum
believed to be analogous to the santorinicele , which is sometimes seen in those with pancreas divisum
Choledochoceles may be successfully managed with endoscopic sphincterotomy, surgical excision, or both, in symptomatic patients.
Type IV
Multiple communicating intra- and extrahepatic duct cysts:
second most common type of bile duct cysts (10%)
-
subdivided into subtypes:
type IVa: fusiform dilation of the entire extrahepatic bile duct with extension of dilation to the intrahepatic bile ducts
type IVb: multiple cystic dilations involving only the extrahepatic bile duct
Type V
Also known as Caroli disease, which is a rare form of congenital biliary cystic disease manifested by cystic dilations of intrahepatic bile ducts. Association with benign renal tubular ectasia and other forms of renal cystic disease.
Additions to the classification
Some authors have coined a "type VI" bile duct cyst, an entity that is considered rare and not part of the original Todani classification. This nomenclature is not widely accepted but is included for completeness.
Type VI
A rare entity describing isolated dilatation of the cystic duct 4,6. Some authors consider this description to be type VIa, while also defining a type VIb that also involves dilatation of the common bile duct 6.
History and etymology
The Todani classification (1977) arose out of the earlier Alonso-Lej classification (1959). The Todani classification added type V (Caroli disease) to the earlier classification. It was developed by the Japanese pediatric surgeon Takuji Todani et al. in 1977 6.
The Todani classification scheme has been called into question in the surgical literature, with claims that it may inaccurately link multiple distinct processes into a spuriously coherent grading scheme 2,3. Specifically, it is questioned whether types II, III, and V are pathophysiologically related to I and IV. Some also think the difference between I and IV may be artificial.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.