
Presentation
10 days post-operative total thyroidectomy for multinodular goiter with fever and discharge from the wound.
Patient Data







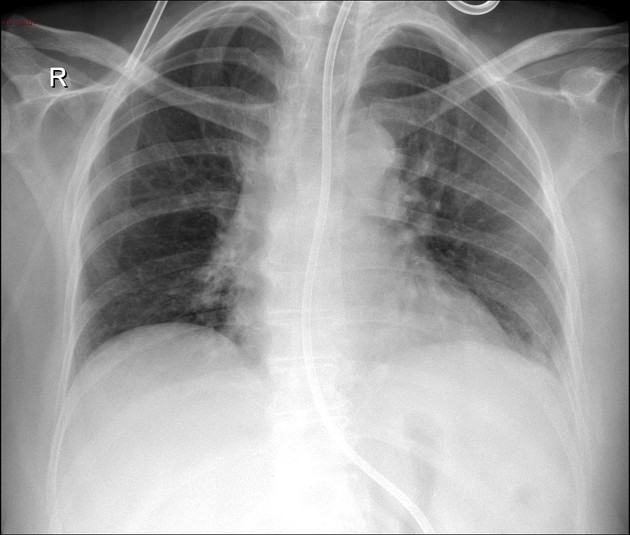
Status post total thyroidectomy showing postoperative changes in the form of diffuse subcutaneous thickening and two surgical drains are seen within the operative bed in anterior lower neck regions.
Endotracheal and NG tubes are seen in situ.
Unremarkable the rest of supra and infrahyoid neck soft tissue spaces.
Diffuse smudged mediastinal fat planes and areas of fluid density disseminated in the mediastinal compartments with faint marginal enhancement are seen, encasing the SVC which showed filling defect within possible thrombosis associated with an enlarged necrotic subcarinal lymph node.
Bilateral subsegmental posterior consolidation and multiple patchy areas of ground-glass density scattered in both lungs suggestive of inflammatory changes.
Bilateral mild pleural effusions are seen.
Lungs are clear. Normal cardiothoracic ratio. No evidence of pleural effusion. Intact bony thoracic cage.
Case Discussion
The postoperative status with above mentioned findings were suggestive of sequelae of an inflammatory process of mediastinitis for clinical correlation and the patient was treated medically.
The diagnostic confirmation by CT of mediastinitis is very important to prevent morbidity and mortality of late diagnosis. So it is essential to know the different characteristic signs of acute mediastinitis and its causes.
The three most common causes of acute mediastinitis are:
- post-surgical: most common cause of mediastinitis, mainly after cardiac curgery, with an incidence of 0.4-5%
- esophageal perforation
- descending necrotizing mediastinitis


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.