
Presentation
The baby did not cry and experienced seizures following delivery. The patient was full-term and was admitted to the ICU of a general hospital, where multiple seizures were noted. Additional information is being sought, although the perinatal history is not particularly informative. The APGAR score, along with all the mentioned history, will be provided low.
Patient Data
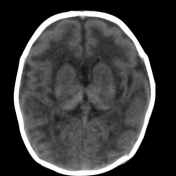

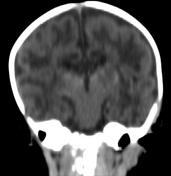
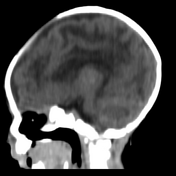
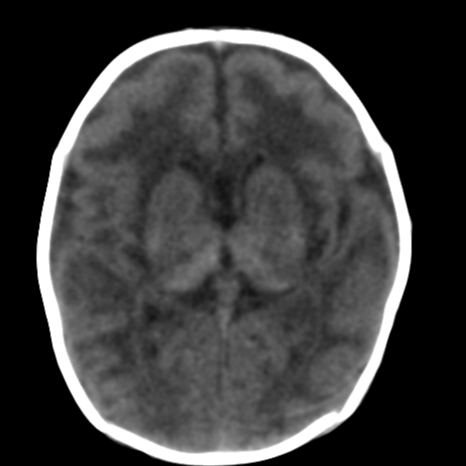
An injury to the grey matter (thalami and partially lentiform nuclei) is indicated by hyperdensities at both thalami and part of the putamens, which is consistent with neonatal hypoxic-ischaemic encephalopathy (HIE). Additionally, there are diffuse oedematous changes within the white matter of the cerebral hemispheres bilaterally.
The findings, supported by the medical history, indicate a diagnosis of neonatal hypoxic-ischaemic encephalopathy (HIE).
Case Discussion
Please take note of the following information:
CT is not the most effective method for evaluating HIE due to the limited ability to distinguish brain tissue in the neonatal brain, which has a high water and cerebrospinal fluid (CSF) protein content.
Recommendations:
consider Krabbe disease when observing bilateral thalamic or basal ganglia (BG) hyperdensity on CT in an infant ¹
suspect prenatal HIE with recovery or inborn errors of metabolism if the imaging findings don't match the patient's history ¹
Protocol note:
Standard MR imaging may be limited by the underdevelopment of myelin and increased water content in the neonatal brain ¹.
Although an MRI has not been performed yet to confirm the diagnosis, patterns of neonatal hypoxic–ischaemic brain injury, particularly isolated thalamic hyperdensity, have been observed along with supported history of recurrent siezures and lack of crying post delivery in addition to post delivery I.C.U admission along with evidence of periventricular leukomalacia(PVL) 1 in this full-term neonate ,collective evidences supporting the most certain diagnosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.