
Presentation
One week history of retrosternal chest pain, dry cough, and generalised fatigue.
Patient Data

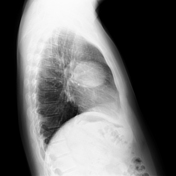
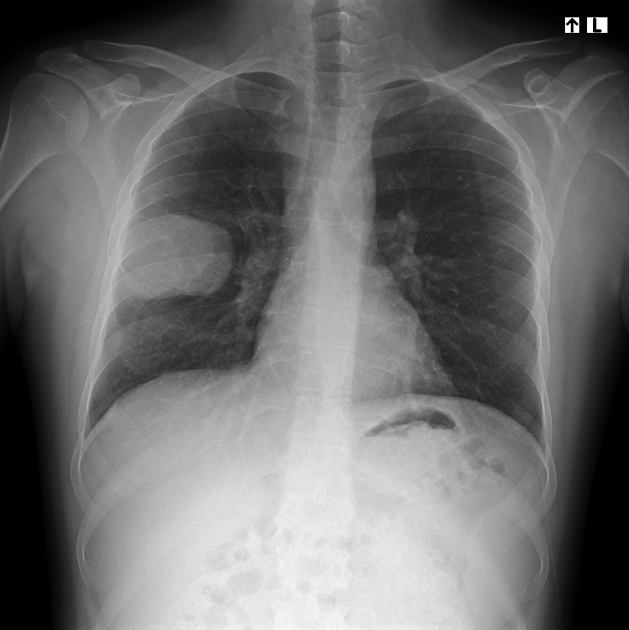



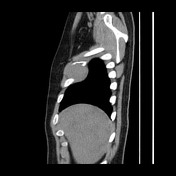


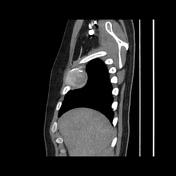


A heterogeneously enhancing, well-demarcated soft tissue mass in the right anterolateral chest wall, containing internal calcific foci. The mass involves the right 4th rib which demonstrates focal expansion and destruction, consistent with a bone-origin tumour. Laterally, it invades the right internal and external intercostal muscles and closely abuts the right serratus anterior muscle without clear evidence of invasion.
The mass indents the adjacent right middle lobe, resulting in areas of subsegmental atelectasis. Lungs are otherwise normal. No pleural effusion.
No pathologically enlarged mediastinal or axillary lymph nodes. No metastases.
Case Discussion
The chest X-ray and CT scan revealed a chest wall mass which was biopsied and identified as a spindle cell tumour without atypical features. Spindle cell tumours are soft tissue tumours that can arise in bone and range from benign to malignant.
In a multidisciplinary meeting, it was decided to excise the tumour along with the 3rd to 5th ribs and perform chest wall reconstruction. Post-surgery, pathology confirmed a spindle cell neoplasm with a Ki-67 index of 5%, indicating low proliferative activity. Additional resection of the serratus anterior muscle was planned to ensure wider surgical margins.
Spindle cell neoplasms with a Ki-67 of 5% generally include benign or low-grade tumours, such as solitary fibrous tumours, fibromatosis, neurofibromas, leiomyomas, and desmoplastic fibromas as well as low-grade spindle cell sarcomas. Spindle cell tumours that arise in bone may be classified as pleomorphic undifferentiated sarcomas, fibrosarcomas or leiomyosarcomas.
Discussion with the pathologist based on radiological features suggests a higher likelihood of a low-grade sarcoma than other differentials.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.