
Presentation
The patient has known Graves disease and a history of thyroid nodules. For ongoing monitoring of known thyroid nodules.
Patient Data

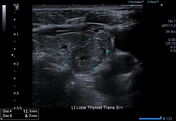
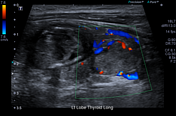
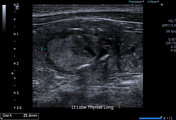
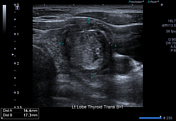

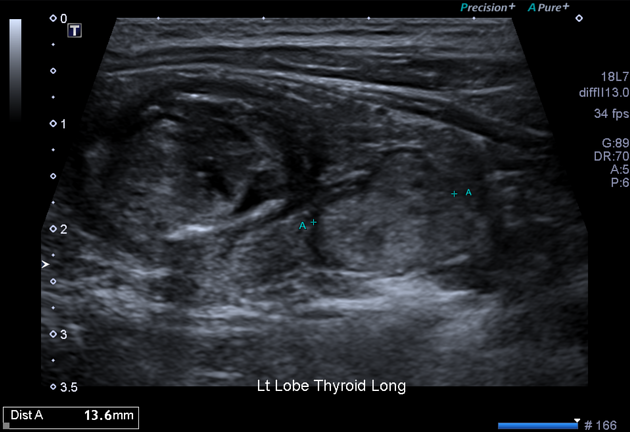
Within the left lobe of the thyroid gland, there are 2 nodules:
mid pole: 17 x 17 x 25 mm, hyperechoic, wider than tall with internal microcalcifications and smooth margins, consistent with a TR4 lesion
lower pole: 12 x 9 x 14 mm, hyperechoic, wider than tall with internal microcalcifications and smooth margins, consistent with a TR4 lesion.
Recommendation
Given the size, it was recommended that the lower pole lesion receive a follow-up scan however the mid-pole lesion warrants a fine-needle aspirate sample (as per ACR TI-RADS).


The thyroid gland is present and entirely suprasternal. The left lobe is mildly larger compared to the right.
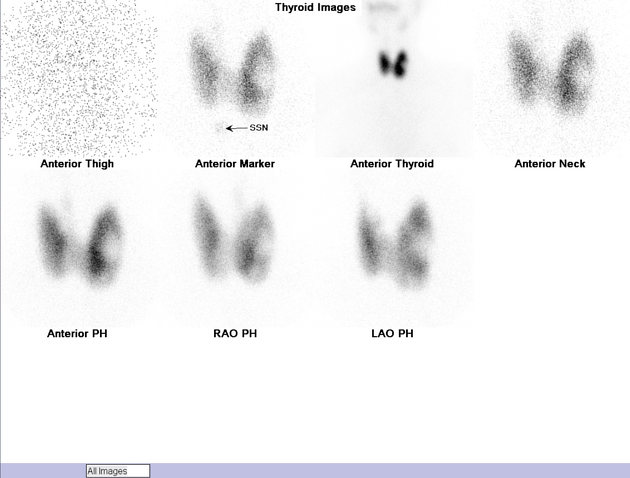
There is markedly increased and diffuse uptake of radiotracer throughout the thyroid gland of 4.9% (Normal 0.5-2.0). The neck-to-thigh ratio is also elevated measuring 32.
There is a focal region of decreased radiotracer uptake within the mid-pole region of the left thyroid gland which indicates a hypo-functioning/cold nodule.
Recommendation:
The hypo-functioning or cold nodule corresponds to the focal mid-pole TR4 lesion identified on the above ultrasound and a fine needle aspirate was recommended.
Case Discussion
The patient was diagnosed with a hypo-functioning cold nodule on a background of Graves disease and was recommended to receive a fine needle aspirate. The histopathology results showed benign follicular cells with no features of thyroid carcinoma.
Fortunately, this case returned a benign result but 10-15% of cold nodules on thyroid scintigraphy are malignant and generally require biopsy1. Correlation with ultrasound is generally recommended to ensure there is a focal lesion that is amenable to biopsy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.