
Presentation
Dysphagia (difficulty swallowing) and dysphonia (hoarse voice).
Patient Data
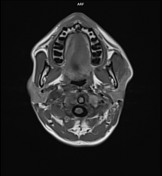

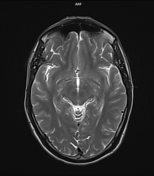
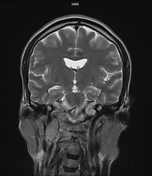
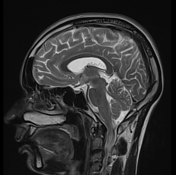
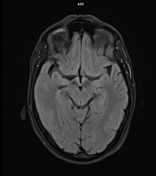
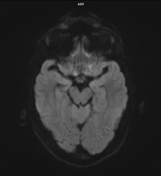

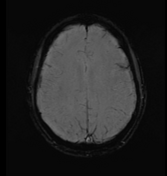
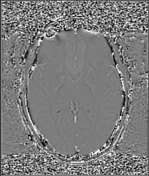
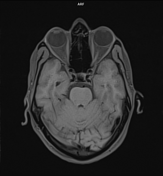
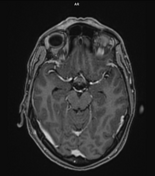
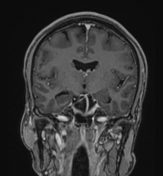
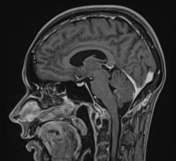
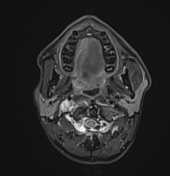
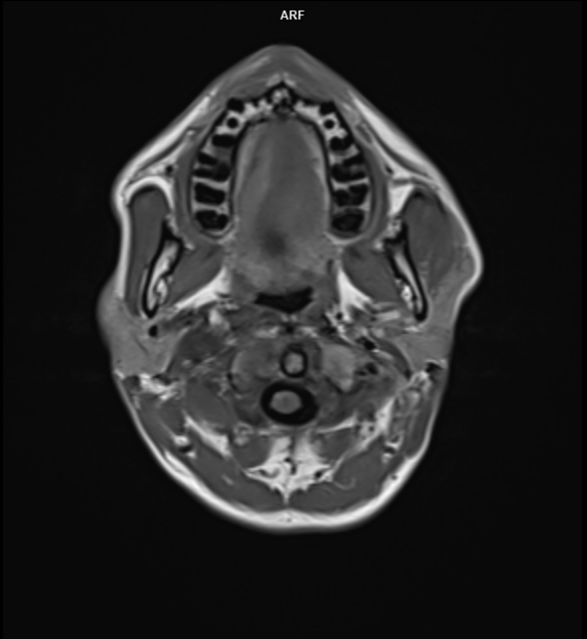
There is an irregular-shaped lobulated mass lesion of measuring ~6.0 x 3.0 x 3.4 cm (CC x TR x AP) in the right jugular fossa with resultant mild-to-moderate widening of the jugular foramen. The lesion has both extracranial and intracranial extra-axial components. The lesion is extends superiorly up to the cerebellopontine angle (CPA) cistern region and abuts the CN VII/VIII complex, right vertebral artery, ipsilateral cerebellar hemisphere, and medulla oblongata, without evidence of mass effect on it. Inferiorly, the lesion extends up to the C2 vertebral level. Medially, the lesion extends below the ipsilateral longus colli muscle, reaching up to the midline and anteriorly causing partial encasement (~120 degrees) of the internal carotid artery. The internal jugular vein is compressed by the mass lesion and cannot be delineated separately. The lesion appears iso- to hyperintense on T2W/FLAIR images with no evidence of diffusion restriction on DWI. Multiple tiny hyperintense foci on T1W images with corresponding blooming on GRE and hyperintensity on filtered phase images, suggesting hemorrhages/vascular flow voids (salt-and-pepper appearance). Marked heterogeneous enhancement seen on postcontrast images.
There is significant atrophy of the right sternocleidomastoid muscle, mild right vocal cord edema, and edema and fatty atrophy of the right half of the tongue muscle, likely due to involvement of CN X, XI & XII by the mass lesion, respectively .
Remaining portions of the brain are unremarkable.
Case Discussion
Collet-Sicard syndrome is a constellation of cranial nerve palsies (CN IX, X, XI & XII) due to a neoplastic or non-neoplastic lesion at the jugular foramen. In this case, a jugular paraganglioma is the culprit.
Co-author: Dr. Avijit Kashyap, Neurosurgeon.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.