
Presentation
Known Crohn's disease.
Patient Data







Findings:
Inflammation
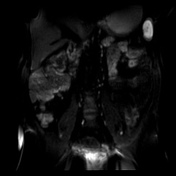
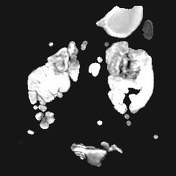
segmental mural bilaminar hyperenhancement and moderate to severe asymmetric wall thickening accentuated along the mesenteric border with a corresponding hyperintense signal on T2w and high signal in diffusion-weighted images (b800)
located in the mid, distal and terminal ileum
small ulcerations
long stricture with intermittent pseudosacculations along the anti-mesenteric border in the distal ileum
Penetrating disease
sinus tracts in the ileum in the mid and left lower abdomen
no complex fistulas, abscess or an inflammatory mass
Mesenteric inflammation
signs of fibrofatty proliferation
engorged vasa recta
no signs of adenopathy
Other findings/complications
- mobile caecum cranially reverted
no signs of mesenteric venous thrombosis or occlusion
no signs of primary sclerosing cholangitis (PSC)
no gallstones or kidney stones
no signs of avascular necrosis (AVN)
Periarticular fatty deposition in the sacrum and bony bridging of the left sacroiliac joint indicative of chronic sacroiliitis
Impression:
Active inflammatory small bowel Crohn’s disease in the mid/distal and terminal ileum with luminal narrowing/strictures and ulcerations.
Small blind-ending sinus tracts can be seen in the affected segment in the left and mid-lower abdomen.
A dedicated pelvic MRI was recommended for the assessment of perianal complications.
Signs of chronic left-sided sacroiliitis.
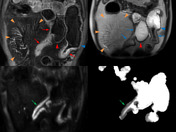
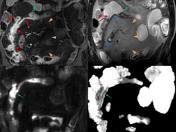
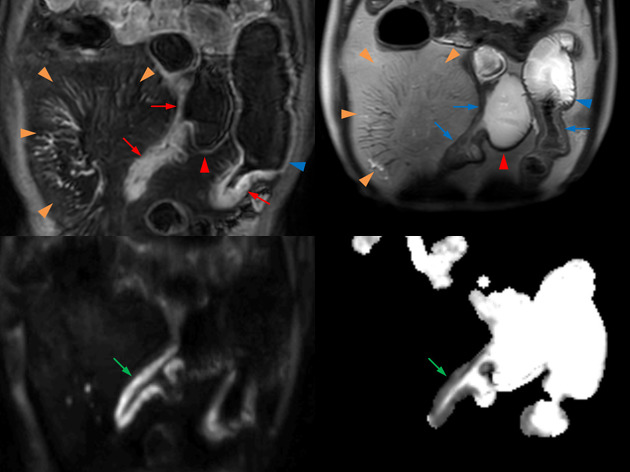
Inflammation
segmental mural hyperenhancement (red arrows)
moderate to severe asymmetric wall thickening accentuated along the mesenteric border (blue arrows)
hyperintense signal on T2w and signs of restricted diffusion on b800 and respective ADC images (green arrows)
Stricture
luminal narrowing/obstruction with signs of active inflammation and with upstream dilatation (blue arrowhead)
Ulceration
small focal break in the intraluminal surface of the bowel wall (green arrowhead)
Pseudosacculation
broad-based outpouchings usually along the anti-mesenteric border (red arrowhead)
Penetrating disease
blind-ending sinus tracts in the distal ileum (orange arrow)
Mesenteric inflammation
signs of fibrofatty proliferation (“creeping fat”) consistent with an increased amount of mesenteric fat adjacent to the abnormal small bowel loops most prominent on the mesenteric border (orange arrowheads)
engorged vasa recta (“comb sign”)
Additional findings
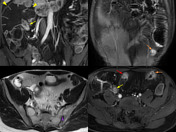
cranially reverted mobile caecum (yellow arrowhead)
inflammatory changes of the terminal ileum (yellow arrow)
sacroiliitis with a bony bridge (purple arrowhead)
Case Discussion
This is a typical case of Crohn’s disease and aims to review typical findings of the disease found on MR enterography (MRE).
On endoscopy, only the terminal ileum showed signs of inflammation and an ulcer with histologically confirmed chronic and florid ulcerations and eosinophilia consistent with Crohn’s disease.
The colon was unremarkable on colonoscopy, which is also reflected by the MRI.
MR enterography (MRE) is able to demonstrate findings in the small bowel that depicts mesenteric findings and penetrating disease (in this case sinus tracts) as well as extraintestinal complications (in this case sacroiliitis).
An additional pelvic MRI (not shown) confirmed the left sacroiliitis but did not show any significant perianal complications such as a fistula or an abscess.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.