
Presentation
History of recurrent urinary tract infections.
Patient Data
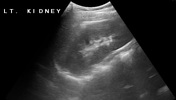





normally positioned average size left kidney
empty right renal bed
relatively small right kidney seen in the lower central abdomen, separate from the left kidney

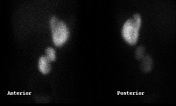

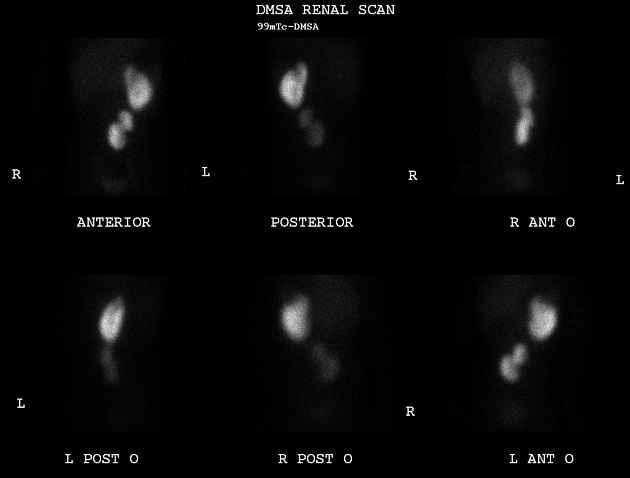
left kidney is seen at its normal anatomical position and shows non-homogeneous distribution of the radiotracer. A cold area suggestive of scarring, is noted at its upper lateral pole
right kidney is visualized in the midline and slightly to the left of the lower abdomen. It is relatively small in size and shows reduced non-homogeneous radiotracer uptake. A cold area suggestive of cortical scarring, is seen at its upper pole. No fusion is seen between the kidneys
differential function: Left kidney contributes 75% while right kidney contributes 25% of total renal function







grade 2 vesicoureteric reflux on the right side (reflux up to the renal pelvis)
grade 1 vesicoureteric reflux on the left side (limited to the lower ureter)













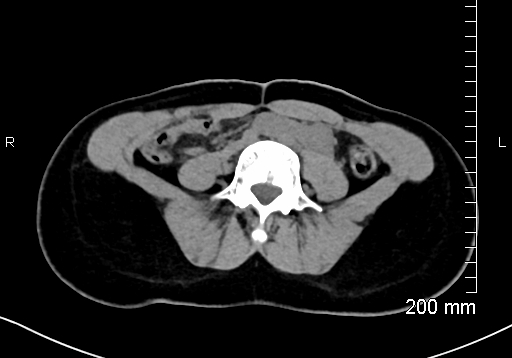
ectopic and malrotated right kidney seen in the midline and slightly to the left of the lower abdomen at L3-L5 level. Normally-positioned left kidney. Both kidneys measure ~9 cm in craniocaudal direction. No communication or fusion is seen between both kidneys
renal cortical defect with focal caliectasis noted at the upper pole of the left kidney.
no radiopaque renal/ureteric calculi or hydroureteronephrosis is seen. Well-distended urinary bladder has smooth outlines.
enlarged and dysplastic left-sided L5 transverse process (type 1a lumbosacral transitional vertebra).
Case Discussion
Imaging findings consistent with crossed renal ectopia. Renal cortical defect at the upper pole of the left kidney demonstrated by both DMSA scan and CT scan. No cortical defect seen in the right kidney on CT scan. Cortical defect seen in the right kidney on DMSA scan was likely attributed to the malrotation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.