
Presentation
Chronic diabetes. Swollen left great toe with an open wound.
Patient Data






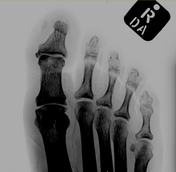
There is soft tissue disruption and an open wound /ulcer relating to the left first-digit terminal phalanx.
There is associated soft tissue swelling of the first ray.
There is background calcified vascular plaque consistent with the history of chronic diabetes.
There is incidental symphalangism involving the 2nd to the 5th digits.
There are no sinus tracts, no periosteal reactions, and no bone erosion to suggest a site of osteomyelitis or septic arthritis.
There is age-appropriate OA.
There is incidental Achilles insertional enthesopathy and degenerative plantar calcaneal spurring.
There is an incidental turret exostosis.






On a PACS search, there is a prior visit of approximately 1 year before the current presentation.
Unusually the history is similar. The patient presents with swelling of the right 1st digit with a clinical suspicion of cellulitis.
Plain films confirm a swollen first toe, vascular calcified plaque, and 2nd to 5th-digit symphalangism.
There is degenerative plantar calcaneal spurring and Achilles calcific tendinosis.
There is age-appropriate OA.
Case Discussion
A case of dual clinical visits 1 year apart for diabetic foot soft tissue sepsis/cellulitis of the first digit, that was successfully treated and resolved with aggressive intravenous antibiotics on both occasions. The presence of osteomyelitis and septic arthritis must always be considered and excluded both clinically and on imaging (MRI / Nuclear scintigraphy). In this instance, the plain films were negative in this regard, as is often the case early on in the clinical presentation.
There is incidental symphalangism of the 2nd to 5th digits bilaterally.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.