
Presentation
Sudden onset expressive dysphasia and right sided weakness
Patient Data
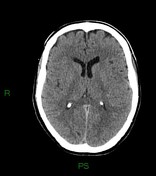

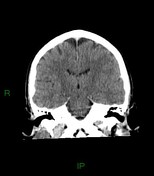


There are a few areas of high attenuation in the left parietal lobe in keeping with acute haemorrhage. Minimal perihaematomal oedema. No subarachnoid or intraventricular haemorrhage. No significant mass effect. No evidence of acute infarct.
The superior sagittal sinus appears hyperdense at the vertex, as do several left side cortical veins including the left superior anastomotic vein. A right sided cortical vein overlying the frontal lobe is also hyperdense.
The findings are in keeping with small parietal haemorrhages secondary to venous sinus and cortical vein thrombosis.
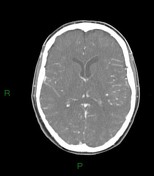
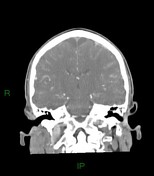

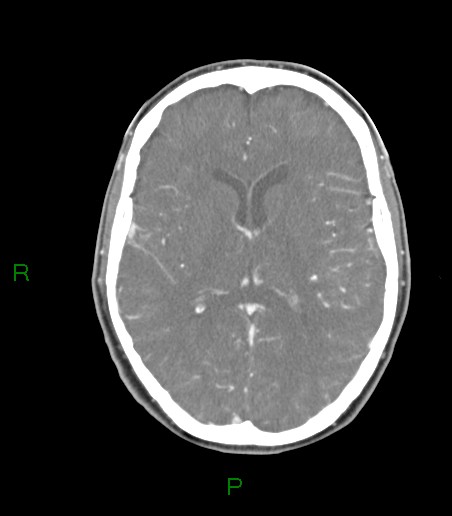
There is an extensive filling defect in the superior sagittal sinus extending to the torcula and proximal right transverse sinus consistent with thrombus. There is no opacification of the cortical veins which were hyperattenuating of the non contrast CT.
The inferior sagittal, straight and sigmoid sinuses opacify normally, as do the deep and internal cerebral veins.
Case Discussion
- Macrovascular lesions, such as venous thrombosis, underlie 10-15% of spontaneous intracerebral haemorrhage.
- Early identification of such abnormalities is important to allow appropriate treatment.
- Specific features on non contrast CT of an underlying macrovascular lesion include hyperdense dural venous sinuses and cerebral veins.
- Thrombosed cortical veins can be overlooked on CT venograms due to the lack of enhancement, close position to the skull and variable course. Correlation with a non contrast CT helps identify non-opacified thrombosed cortical veins on CT venogram.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.