
Presentation
Fever and dyspnoea during hospitalisation
Patient Data




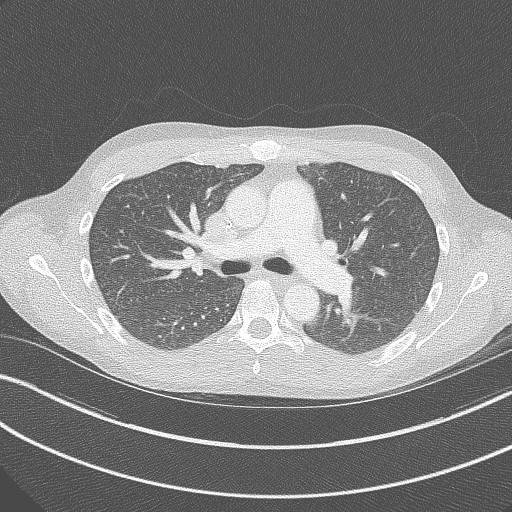
Diffuse tiny ill-defined ground-glass centrilobular nodules involving both lungs.
Dilated pulmonary trunk (3.3 cm) and dilated right heart cavities, in keeping with pulmonary arterial hypertension and right heart strain.
Adequately placed right PICC.
Upper abdomen shows signs of known cirrhosis with portal hypertension and chronic pancreatitis.


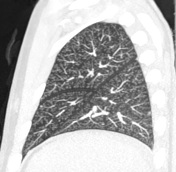
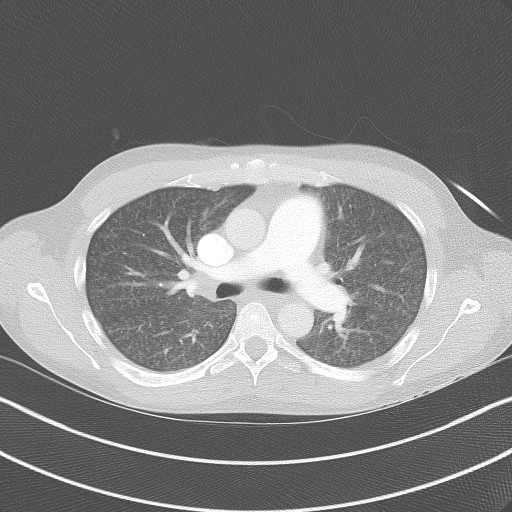
Diffuse centrilobular nodules are now more clearly seen, with an obvious tree-in-bud pattern with subpleural and peri-fissural sparing, best seen on MIP reformats.
Deteriorated acute pulmonary arterial hypertension. The pulmonary trunk now measures 3.6 cm. The right ventricle and atrium are even more dilated than previously, with new dilatation of the IVC and contrast reflux in the hepatic veins.
New multi-segment scattered zones of consolidation of unknown aetiology.
Initially, nodules were described as a miliary pattern, prompting a search for an infectious cause. Additionally, right heart strain was not reported.
Case Discussion
Patient was known for opioid use disorder, alcoholism and prior hepatitis C infection. During hospitalisation for attempted detox, he developed acute respiratory distress. Initial CT was interpreted as having miliary lung nodules suggestive of infectious disease. Subsequent CTPA was negative for pulmonary embolism but showed progression of what was now clearly identified as a centrilobular pattern of micronodules and progressive right ventricular strain. However, an infectious aetiology was still deemed to be most likely, such as diffuse infectious bronchiolitis, with possible superimposed septic emboli to explain the new areas of consolidation.
Only later on further review of CT studies was the combination of diffuse tree-in-bud (centrilobular) nodules and acute pulmonary hypertension proposed to be most likely related to excipient lung disease. Patient was further questioned and observed, and found to have been crushing hydromorphone pills and injecting them through his PICC. Transbronchial lung biopsy showed multiple intravascular foreign body granulomas surrounding refractile synthetic material, compatible with intravenous foreign body injection.
On serial follow-ups for two years (at time of writing), patient remained with diffuse tree-in-bud nodules, but right heart function partially improved. Interestingly, at the time of initial presentation, patient was confirmed by brain MRI to have had recent cerebral embolic infarcts. Echocardiography showed a patent foramen ovale with right-to-left shunting, likely because of the acute right heart strain caused by his excipient lung disease, with reversal of the normal pressure gradient between left and right atria.
This case's main teaching points are the following:
- Though diffuse tree-in-bud/centrilobular nodules are mostly related to a bronchiolar branching pattern, rarely they might be secondary to an intravascular process such as injected foreign bodies or tumour emboli. Remember that in the secondary pulmonary lobule, pulmonary arteries follow the same branching pattern as terminal bronchioles.
- When combined with acute pulmonary hypertension, diffuse tree-in-bud nodules are highly suggestive of excipient lung disease, whereas most other aetiologies of tree-in-bud nodules do not cause right heart strain.
- When diffuse micronodules are present, subpleural and peri-fissural sparing suggest a centrilobular pattern rather than miliary pattern.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.