
Presentation
Diabetic patient presented with abdominal pain, high lactate and constipation.
Patient Data


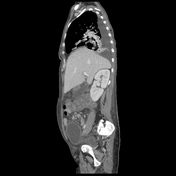


A large mural defect is seen at the gastric fundus and greater curvature with fistulous communication into a large collection replacing most of the splenic tissue, in keeping with gastro-splenic fistula, a sequel of severe infective process.
Associated with elevated left hemi-diaphragm, which is seen as inseparable from the aforementioned gastro-splenic fistula and collection, with suggestion of left hemi-diaphragmatic defects.
Hepatomegaly, with multiple small hypodense liver lesions, likely small abscesses.
Mild loculated left pleural effusion with enhanced pleural surface, denoting left pleural empyema.
Moderate right pleural effusion.
Bilateral lung lower lobe and lingula collapse consolidations with air bronchogram, likely representing chest infection with aspiration.
Diffuse enlargement of the thyroid gland.
Case Discussion
Intraoperative gastrosplenic fistula was found, partial gastrectomy and splenectomy were done and the pathology specimen revealed gastric and splenic suppurative infection with Mucormycosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.