
Presentation
Chronic left groin pain and paresthesia spreading to the scrotum and the medial aspect of the left thigh.
Patient Data
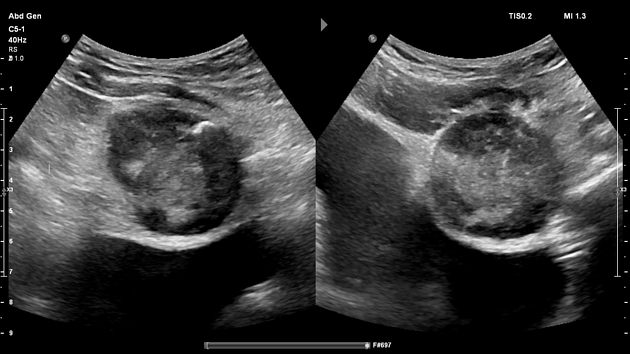
Pelvic ultrasound revealed a well-defined oval solid mass with heterogeneous echotexture, mostly hypoechoic with a peripheral eccentric calcification. PW showed a low resistance monophasic flow with a PSV less than 20 cm/s. The mass, measuring 43x41x51 mm, is centered in the left pelvis and exerts mass effect on the urinary bladder pushing its left anterior wall rightward.

Non-enhanced CT images showed a high attenuation pedunculated solid mass in the left pelvis growing between the urinary bladder, left external iliac vessels and the left rectus abdominis muscle which is anteriorly displaced. The inguinal canal is tangentially encompassed by the mass which also compresses the external iliac vein against the iliopsoas muscle with a peduncle pointing toward it. Note the eccentric calcification in the antero-basal portion of the lesion where the mass abuts the postero-medial border of the inguinal canal close to the running course of the genitofemoral nerve where it probably comes from.
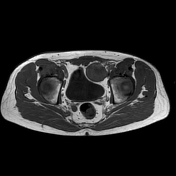

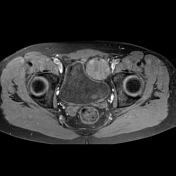
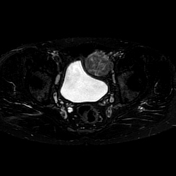
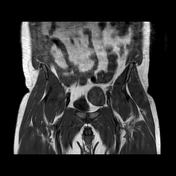
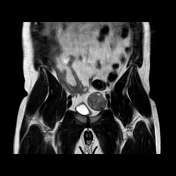
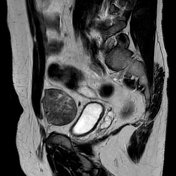
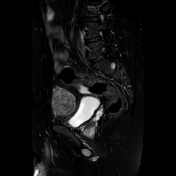
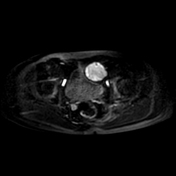
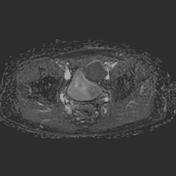
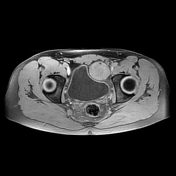
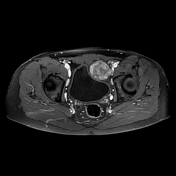
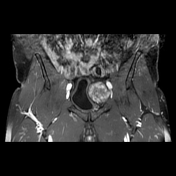
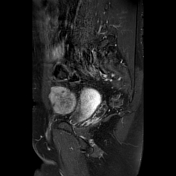

Further evaluation with standard pelvic protocol 1.5 T MRI showed a pedunculated pelvic mass with predominantly low T1 and high T2 signal intensity with intense heterogeneous enhancement.
Multiple small ring-like structures surrounded by T2 hyperintesity (fascicular sign) are suggestive of fascicular bundles within the nerves. Diffusion is restricted and the signal does not suppress on fat saturation sequences.
The mass is well-circumscribed and displaces the adjacent structures with no sign of infiltration or pelvic lymphadenopathy.
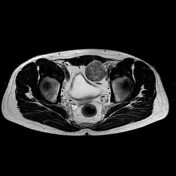
The peripheral punctate hypointensity corresponds to the eccentric calcification best seen on the ultrasound and CT images above.
Given the pelvic location with abundant fat surrounding the lesion, a split fat sign cannot be seen.
Such findings are in keeping with a tumor of neurogenic origin.
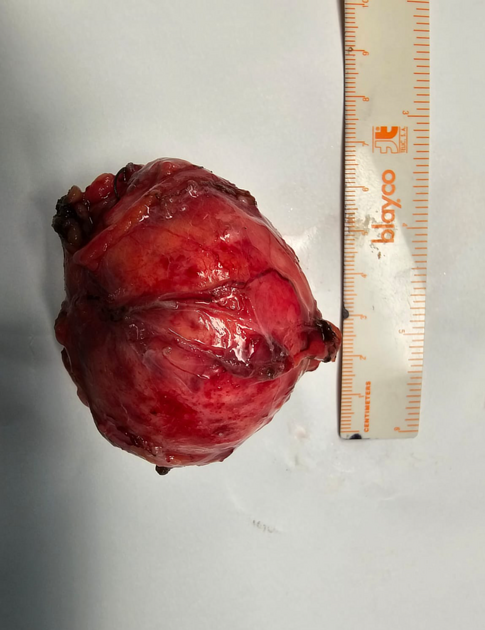
Post-surgical macroscopic tumor appearance demonstrates an encapsulated solid mass measuring about 6 cm in greatest diameter.
This image is courtesy of the surgical team: Prof. Asc. Dr. Ridvan Alimehmeti and Dr. Denis Godaj
Histology
Features of fusiform neoplastic process cells with ovoid or elongated moderately deep-colored nuclei, leptophyte chromatin, with indistinct cell boundaries and without visible nuclei. No atypia or mitoses were seen. Cells were found in a collagenous substrate arranged in bundles often intertwined with each other and to a lesser extent in small and indistinct swirling formations with relatively sparse allocation of individual feeder cells.
Immunohistochemistry
Several neoplastic cells showed S100 positivity, whereas the opposite neoplastic cells were negative for SMA, Desmin, SOX10, c-kit, CD34, CD99, STAT6 and MUC4. About 2% of the nuclei of neoplastic cells show positivity for the mitotic marker Ki-67.
Case Discussion
A case of biopsy-proven genitofemoral nerve schwannoma in a middle-aged, otherwise healthy man presenting with vague, chronic pelvic pain and numbness extending to the scrotum and thigh, worsening over the past three months.
Multimodal imaging appearance is highly suggestive of schwannoma. The typical signal intensity in different sequences, the enhancement pattern and the fascicular sign observed on T2WI support the diagnosis. The lesion was biopsied in another hospital, which confirmed the diagnosis.
Schwannomas are common benign tumors arising from the schwann cells of the peripheral or cranial nerves, but a pelvic location is rare. The patient underwent surgical resection with complete tumor removal.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.