
Presentation
Brought in by ambulance with GCS 4 after a head strike. The patient is anticoagulated and taking clopidogrel.
Patient Data





An undisplaced fracture of the left parietal bone extending medially to the lambda propagating through the right lambdoid suture with associated diastasis. Associated large subgaleal hematoma overlying the left parietal/occipital bone. The displaced fracture through the mastoid process of the temporal bone with both a longitudinal and transverse orientation. The fracture extends through the tympanic part of the temporal bone, middle ear and into the temporomandibular joint. Associated right mastoid, right middle and external ear hematoma. Further extension anteriorly through the anterior and posterior walls of the right carotid canal into the body of the sphenoid. No obvious fracture extension into the left carotid canal. No other skull fracture was identified. Subcutaneous emphysema within the right masticator space is noted.
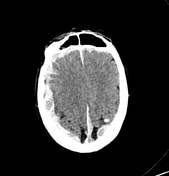
Large epidural hematoma associated with the aforementioned left parieto-occipital skull fracture measuring up to 15 mm in axial dimension. Extensive contrecoup injury characterized by a large right subdural hematoma overlying the right cerebral convexity measuring up to 15 mm. Small subdural hematoma overlying the anterior left frontal lobe and left parietal lobe.
There is significant cerebral edema characterized by uncal hernication with diffuse effacement of the basal cisterns. No tonsillar herniation. Extensive loss of grey-white differentiation throughout the cerebral parenchyma.
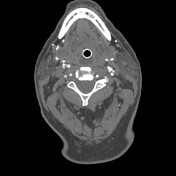


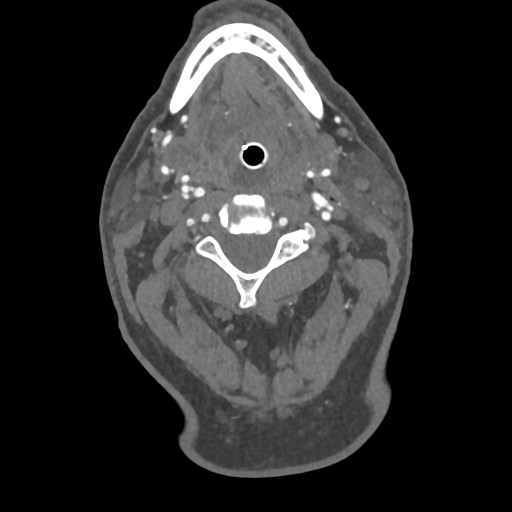
Conventional three-vessel configuration of the aortic arch vessels. No opacification of the terminal segments of the internal carotid arteries bilaterally and at the basilar tip. No flow is demonstrated in the Circle of Willis. This is likely the result of diffuse raised intracranial pressure secondary to catastrophic hypoxic brain injury.
Reduced opacification of the V4 segments of the vertebral arteries, proximal basilar artery, and the petrous and lacerum segments of the internal carotid arteries. There are locules of gas within the right transverse sinus which is concerning for a right transverse sinus injury and potential sinus thrombosis in this region.
Case Discussion
This patient subsequently passed in the department from his catastrophic head injury. No surgical options were available to improve prognosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.