
Presentation
Referred from bowel cancer screening program with positive fecal immunochemical test (FIT).
Patient Data




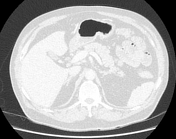
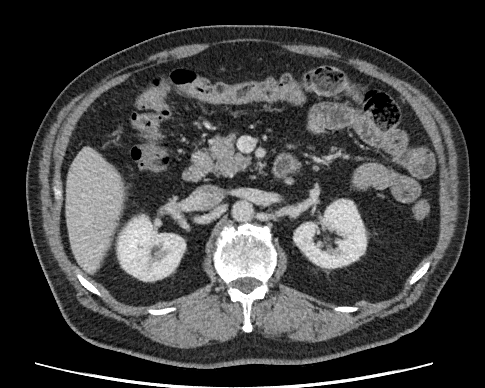
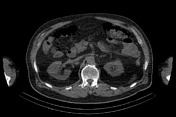
Approximately 3 cm enhancing lesion along the medial wall of the cecum adjacent to the ileocecal valve. Multiple small calcifications (calcified mesenteric lymph node?) are noted adjacent to the cecum. 10 mm mild hypodensity in segment 5 of the liver and 20 mm cyst in the left lobe. No mediastinal, para-aortic or pelvic lymphadenopathy is seen. No suspicious pulmonary or osseous abnormality is seen.
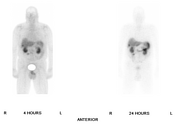

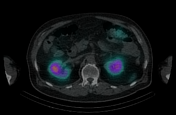
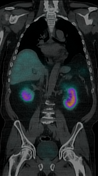
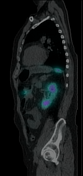


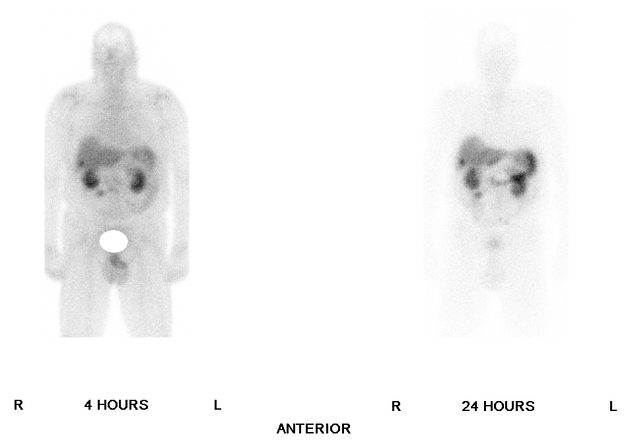
Somatostatin avid lesion along the medial aspect of the cecum, showing focal increased radiotracer uptake. Small focal somatostatin avid lesion, suggestive of metastasis in segment 5 of the liver.
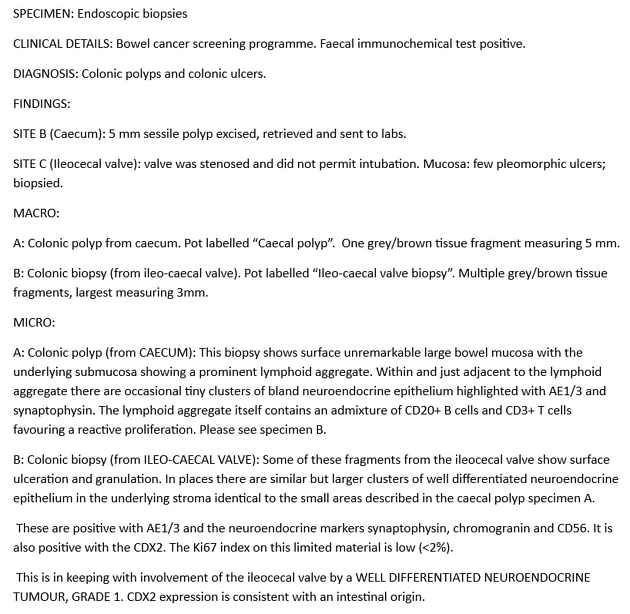
Histopathology report of the colonoscopic biopsies shows well-differentiated neuroendocrine tumor, grade 1. Ki 67 index is less than 2.
Case Discussion
Neuroendocrine neoplasms (NENs) are epithelial lesions with neuroendocrine differentiation and in the small bowel, they are believed to originate from the intraepithelial endocrine cells 1. Gastrointestinal tract NENs are classified into three categories: well-differentiated neuroendocrine tumors, poorly differentiated neuroendocrine carcinomas, and mixed neuroendocrine or nonneuroendocrine neoplasms 1. These categories have distinct biologic activity, which is determined by the mitotic rate, Ki-67 index and degree of differentiation 1. Well-differentiated neuroendocrine tumors are further classified into: grade 1 (mitotic rate less than two mitoses per 2 mm2 and Ki-67 index less than 3); grade 2 (mitotic rate 2-20 mitoses per 2 mm2 and Ki-67 index 3-20) and grade 3 (mitotic rate greater than 20 per 2 mm2 and Ki-67 index greater than 20) 1. Neuroendocrine carcinomas show a mitotic rate greater than 20 mitoses per 2 mm2 and Ki-67 index greater than 20 and are poorly differentiated 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.