
Presentation
An abdominal wall bulge at the site of previous surgery.
Patient Data





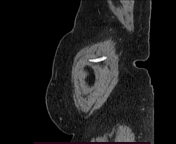


Relatively large ventral abdominal wall facial defect seen straddle the umbilicus with two sacs, the largest on the right of the midline. The hernial sac contains almost all the transverse colon, mid-ileal loops (in the right sac), and small bowel mesentery with minimal fat stranding with no trapped fluid within. No bowel tethering at the defect, and no finding to suggest adhesion, ischemia, or obstruction.
Rectus abdominis muscle thickness of 10-14 mm at the level of the defect and 4-8 mm width with noticeable lateral distensibility, no significant fat infiltration.
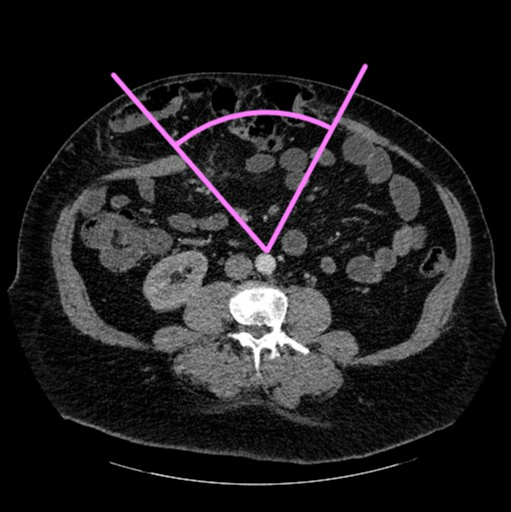
To calculate the component separation index we have to measure the angle of diastasis at the axial CT slice that shows the hernia orifice at its widest. First, draw two lines from the medial edges of the rectus abdominis muscles to meet at the anterior wall of the aorta. The angle of diastasis is the angle between these two lines (the pink angle drawn above, and in our case, it measures about 66 degrees). Second, divide the angle of diastasis by 360 degrees to obtain the component separation index (in our case it measures 0.18). Values more than 0.21 usually predict the need for interpositional mesh repair.
Case Discussion
Ventral abdominal wall hernia, bowel-containing with low component separation index of <0.2, no intestinal obstruction or strangulation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.