
Presentation
Punch to head 10 days ago. Persistent headache since with severe lethargy, weakness, nausea, vomiting. Looks unwell and drowsy.
Patient Data
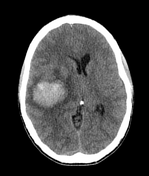

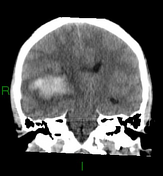
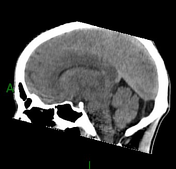
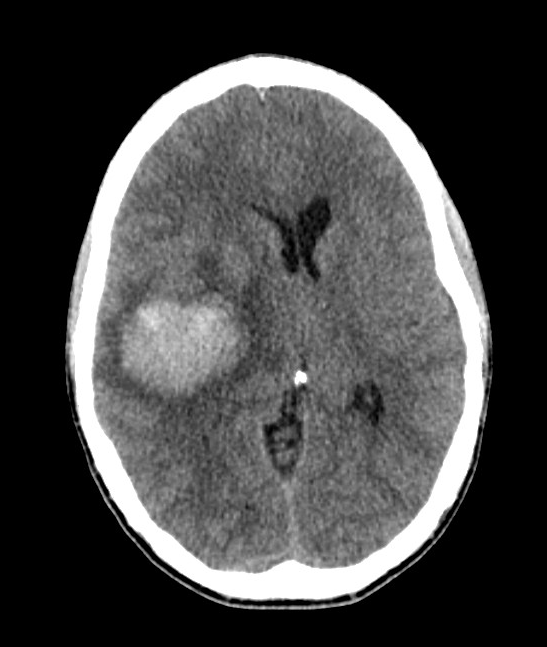
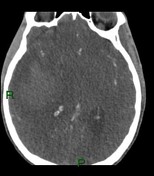
Lobar intracerebral haematoma centred in the right parietal lobe. Its attenuation coupled slightly ill-defined margins are in keeping with a subacute appearance. A small volume of perihaematomal oedema is present. No subarachnoid or intraventricular haemorrhage.
Mass effect with leftward mildline shift and partial effacement of the right lateral ventricle. Temporal horn dilatation in keeping with mild obstructive hydrocephalus.
No areas of calcification or obvious abnormal vessels related to the haematoma.
No evidence of small vessel disease.
CTA performed due to ...
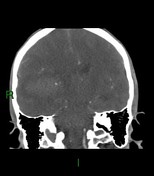
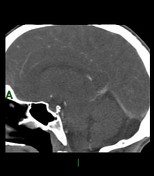

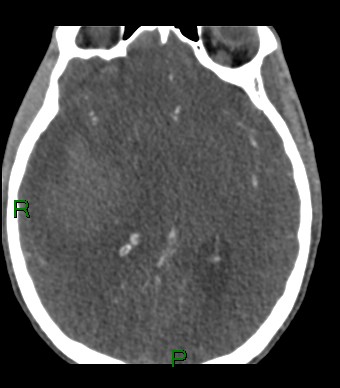
CTA performed due to patient's young age
There are abnormal vessels lying medial to the haematoma. These appear to drain into the vein of Galen, which shows early contrast opacification. The arterial feeders are difficult to identify. The findings are in keeping with an arteriovenous malformation.
A catheter angiogram was performed which confirmed a small right tmeporal lobe arteriovenous malformation with a small nidus in the posteromedial right temporal lobe.
The feeding artery looks to be the right anterior choroidal which may be distorted by the haematoma. It is very tortuous and small and forms a 360 degree loop. The draining vein is deep, into the straight sinus.
Case Discussion
The imaging shows a spontaneous intracerebral haemorrhage secondary to an arteriovenous malformation.
- Macrovascular lesions, such as arteriovenous malformations, underlie 10-15% of spontaneous intracerebral haemorrhage.
- Early identification of such abnormalities is important to allow appropriate treatment.
- Young age is a risk factor for an underlying macrovascular lesion 1,2, and should lead to vascular imaging.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.