
Presentation
History of hypertension. Presented with vomiting and vertigo following exercise.
Patient Data
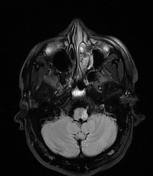

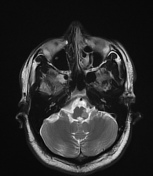
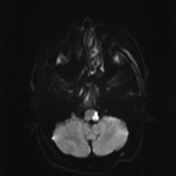
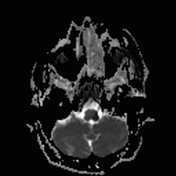
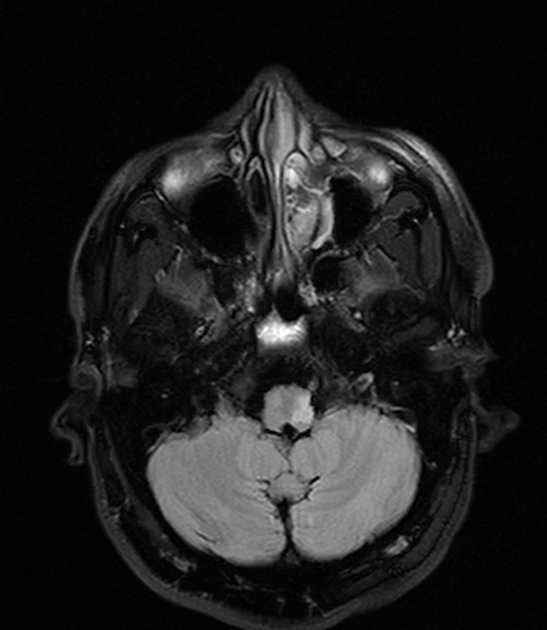
There is an area of high DWI and low ADC signal involving the left side of medulla oblongata suggestive of acute infarction.
A small T2W high signal intensity area is noted in the left middle cerebellar peduncle without diffusion restriction. The rest of the pons and mid-brain show normal signal intensities.
The cerebellum shows no abnormal changes in signal characteristics. There is a small area of high DWI and ADC signal in the left corona radiata and posterior limb of the internal capsule.
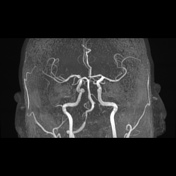
MRA
The left side vertebral artery does not show a normal high signal throughout its course from the origin to the termination, other than a few faint high signals. There appears to be a semilunar low signal intensity flap at the origin of the left vertebral artery. Left PICA is not visualised.
The right side vertebral artery appears normal.
Case Discussion
The lateral part of the medulla oblongata is supplied by the posterior inferior cerebellar artery. It is a branch of the vertebral artery. Thrombosis of one of these arteries produces dysphagia, dysarthria, and thermoanesthesia on the ipsilateral side of the face, vertigo, nystagmus, vomiting, ipsilateral Horner's syndrome, ipsilateral cerebellar signs, and contralateral loss of sensations of pain and temperature.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.