
Presentation
Acute-onset dense left hemiplegia and slurred speech
Patient Data


Brain
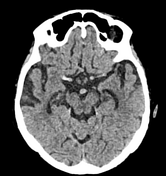
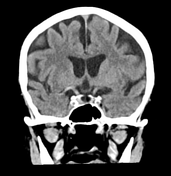
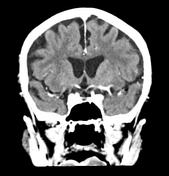
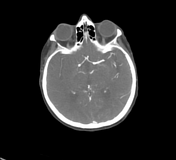
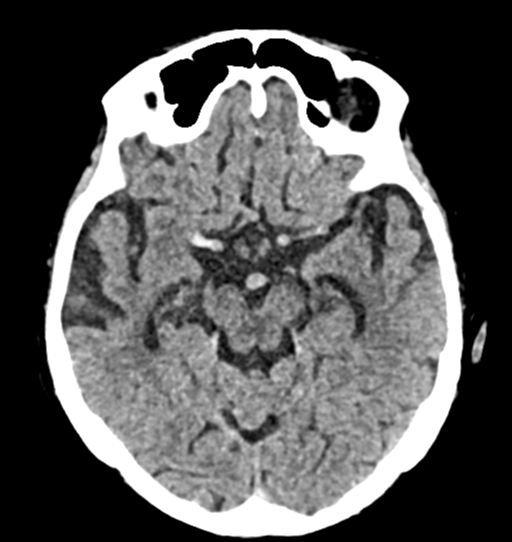
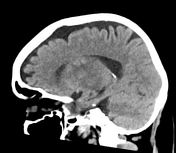
Hyperdense artery sign demonstated within the M1 segment of the right MCA (axial, coronal). Grey-white matter differentiation is preserved. No intra or extra-axial haemorrhage identified. Calcified foci noted within the bilateral basal ganglia. Bilateral periventricular white matter hypoattenuation. Normal ventricular calibre without features of hydrocephalus.
Perfusion
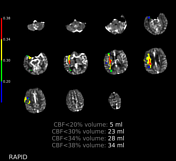
A region of reduced CBF volume <30% (23 mL) in the MCA territory with a corresponding region of increased Tmax >6 seconds (132 mL) is noted in the right frontoparietal lobe. This equates to a mismatch volume of 109 mL, suggesting a large cerebral penumbra.
Angiogram
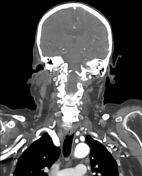
Normal aortic arch branching pattern. Tortuous origin of the right common carotid artery (axial, coronal) with mild stenosis at the right carotid bulb. A filling defect traverses the entire right MCA M1 segment from the origin to the branch point (axial, coronal). Otherwise normal opacification of the anterior and posterior intracrebral circulation.
Normal opacification of the bilateral common carotid, internal and external carotid, vertebral and basilar arteries without appreciable filling defect, aneurysm or stenosis.
Conclusion
Established right M1 segment MCA infarct with a large cerebral penumbra.


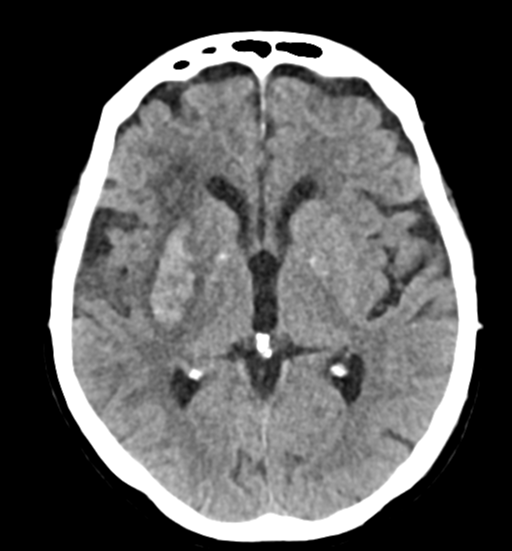
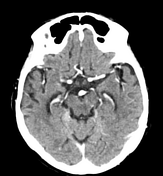
Heterogeneous hyperattenuation surrounding the right basal ganglia and internal capsule consistent with haemorrhagic transformation of the known M1 segment infarct. The haemorrhage mesaures 33 x 16 x 25 mm and displays surrounding oedema. Localised mass effect causing effacement of the anterior horn of the right lateral ventricle.
Persistent hyperdensity of the right distal M1 segment of the MCA. Mild loss of grey-white matter differentiation involving the right insular and temporal cortices with loss of the insular ribbon sign (axial, coronal).
No global mass effect or midline shift. No intraventricular haemorrhage or hydrocephalus. No additional area of infarction or haemorrhage noted.
Case Discussion
This is a case of an 85-year-old female who presented with acute-onset dense left hemiparesis and slurred speech. The lower limb was more affected than the upper limb.
The initial CT stroke protocol was done about 6 hours after symptom-onset which diagnosed acute ischaemic MCA infarction with a large cerebral penumbra.
She was not a candidate for thrombolysis or endovascular clot retrieval (ECR) due to frailty and complex medical comorbidities. Follow-up CT 24 hours later revealed haemorrhagic transformation of the infarcted core. The decision was made for palliation and she unfortunately died the following day.
The radiologic findings of ischaemic stroke exist on a temporal spectrum. Hyperacute findings include the dense artery sign (reflecting fresh thrombus). Haemorrhagic transformation is a later, subacute finding.
Careful interpretation of perfusion imaging is imporant in ischaemic stroke as it measures the size of the infarcted core and also the salvagable penumbra. This is critical in guiding the time-sensitive treatment decision of ECR versus thrombolysis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.