
Presentation
Presented with respiratory distress after birth with poor Apgar score.
Patient Data

endotracheal tube with its tip at the T4 level
nasogastric tube with its tip in the stomach
umbilical vein catheter with its tip at T12 level and rightward deviation towards the liver is observed, likely within the right portal vein or branch
a distended lucency is seen at the retrocardiac region, with no air-fluid level within
stomach and multiple bowel loops are distended
no evidence of spinal segmentation abnormality
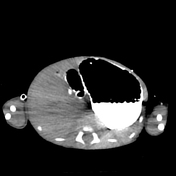



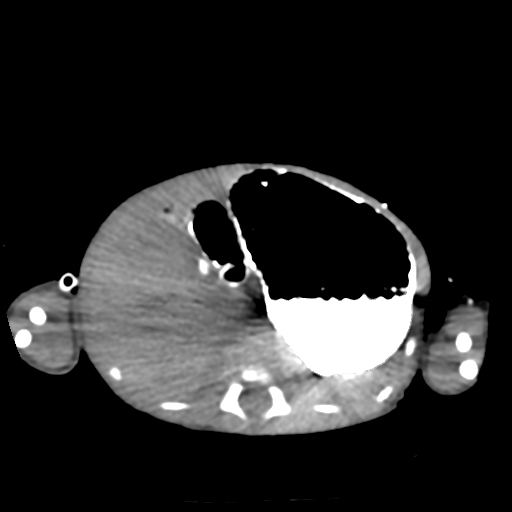
*Suboptimal study due to non-optimization of the intravenous contrast opacification. Dense oral contrast is causing streak artefacts onto the surrounding structures.
Endobronchial and nasogastric tubes are in situ. Dilated esophagus, stomach, and D1 with retained secretions and oral contrast are noted. D2 till D4 are not dilated. No obstructive lesion is identified in the distal esophagus. Dilated esophagus, with deviation of the trachea to the left. The stomach is located below the left hemidiaphragm. Contrast is passed through the esophagus, stomach, and small bowel loops.
No elevation of both diaphragms is seen. Bilateral hemidiaphragms are intact. No herniation of the liver, spleen, or bowel loops into the hemithorax.
Enlarged anterior mediastinum with triangular soft tissue density is in keeping with thymus.

endotracheal and nasogastric tubes are in situ. ECG lead is projected over the right-sided abdomen
the previously seen retrocardiac lucency is no longer identified in this current study
the stomach and small bowel loops are not dilated
subsegmental atelectasis is seen at the right upper zone
Case Discussion
This is a rare case of transient megaesophagus with no CT evidence of congenital diaphragmatic or hiatus hernia.
The patient was a preterm baby at 33 weeks and 5 days, who had respiratory distress syndrome and was admitted to the neonatal intensive care unit (NICU). Chest radiography on day 3 of life revealed a distended retrocardiac lucency, which was not identified in the initial chest radiography on day 1 and day 2 of life. No feeding has been started since birth.
The primary team planned to start the feeding. Therefore, CECT thorax and abdomen were required to confirm the diagnosis of congenital hiatus hernia or congenital diaphragmatic hernia. Surprisingly, a dilated esophagus with retained secretions was found.
Megaesophagus does not commonly occur in neonates. In this case, transient megaesophagus is most likely secondary to motility problems. So far, the patient is currently tolerating well and has no vomiting after starting feeding.
Case co-author: Mr Tan Shung Ken, consultant pediatric surgeon


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}