
Presentation
Right-sided exophthalmos and ophthalmoplegia. Pupil nonreactive to light.
Patient Data
Right parasellar soft tissue mass projecting into the right inferior orbital fissure, the orbital apex, and pterygopalatine fossa. Right Meckel cave obliterated. Erosion in medial aspect of body of greater sphenoid from right middle fossa soft tissue mass. Suspected left petroclival ligament infiltration.
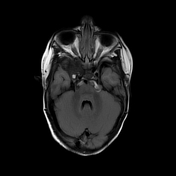

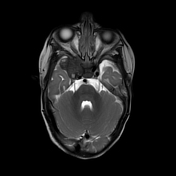
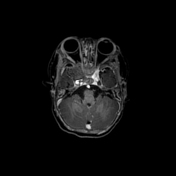
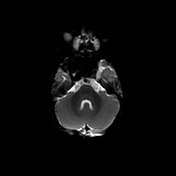
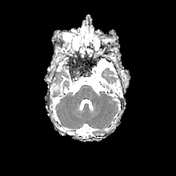
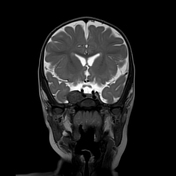

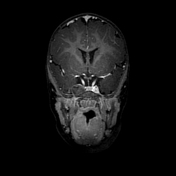
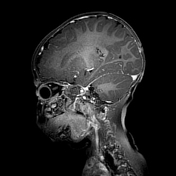
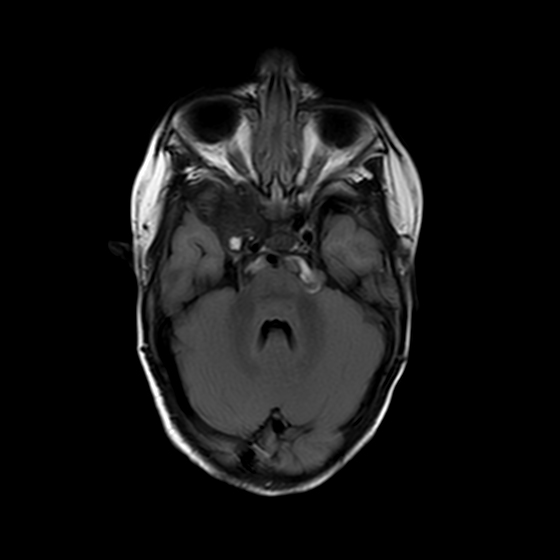
Extra-axial mass in right medial middle cranial fossa, measuring 24 x 17 x 14 (ML x AP x CC) mm, spreading into the orbital apex and widening the optic canal and inferior orbital fissure. Destruction in sphenoid at the posterior part of the orbit and body of sphenoid, both in its right part and at the base of the skull. The optic nerve in the optic canal appears displaced superiorly and compressed. Proptosis, possibly due to orbital wall destruction and exposure to CSF pulsations. The mass displaces and distorts the cavernous sinus and probably invades it. Exerts pressure on the internal carotid artery. Abuts the foramen ovale but does not involve it. Its lateral and superior parts are surrounded by dura mater. Most of the mass elicits low signal on both T1WI and T2WI and enhances weakly. Small component at its posterior part elicits high signal on all sequences Does not restrict on DWI, of low signal on SWI, contains focal calcifications
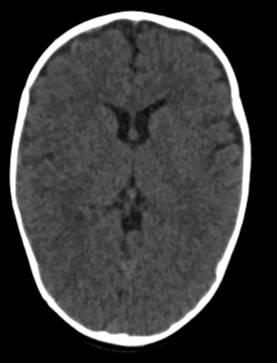
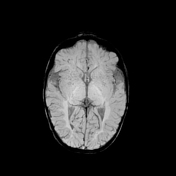
Brain parenchyma normal, ventricles not dilated, no cerebellar tonsillar herniation.
In summary:
Extra-axial right middle cranial fossa mass, invading the orbit and cavernous sinus, surrounded by bone destruction. Taking the congenital disease into account, the mass could represent a metastasis (neuroblastoma, Wilms, hepatoblastoma). There is a high incidence of rhabdomyosarcoma; however, the appearance is not characteristic. Owing to the patient's young age, ATRT cannot be ruled out.
Case Discussion
Proptosis, mydriasis, and ophthalmoplegia of the right eye in an infant with a diagnosis of Beckwith-Wiedemann syndrome.
MRI head showed a right middle fossa tumour.
A biopsy of the mass was obtained - histopathology report:
The mass is composed of small round cells with a hyperchromic nucleus, with barely any cytoplasm. The tumour cells create solid surfaces. In certain areas, there are connective tissue septa covered with tumour cells between which are solid surfaces of cells.
Mitotic activity witnessed.
On immunohistochemical staining, the tumour cells stained positive for myogenin, WT1, and CD56; partially positive for DES, VIM, and SMA; positive in few cells for MYOD1, CD99, EMA, and ALK1; and negative for NSE, SYN, CHR, S100, CD20, CD3, MPX, and PAX5.
Negative for PAX3-FKHR and PAX7-FKHR translocations.
Features compatible with rhabdomyosarcoma, with a differential diagnosis of either embryonal rhabdomyosarcoma or solid variant of alveolar rhabdomyosarcoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.