
Presentation
Irregular menstruation and headache for last the 5 months. Taking PAN-D 40 (combination of pantoprazole and domperidone) for 1month. Serum Prolactin level 95 ng/mL.
Patient Data
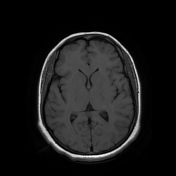

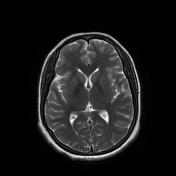
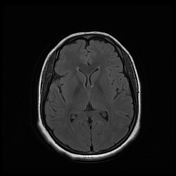
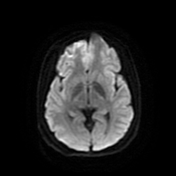
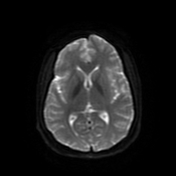
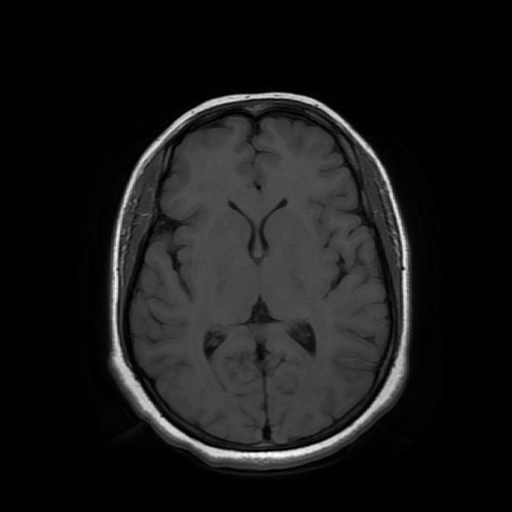
BRAIN:
The ventricles and sulci are normal in size and configuration. There is no acute infarct or intracerebral haemorrhage. No extra-axial blood or fluid collection is present. No intracranial mass is identified. The brainstem, posterior fossa and cervicomedullary junction are preserved. The orbits, periorbital and pericavernous spaces are normal.
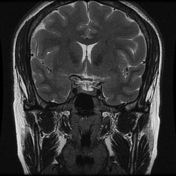
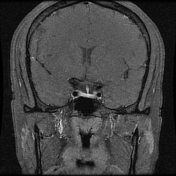
Mucosal thickening is seen in the right maxillary sinus.
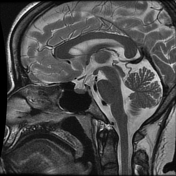
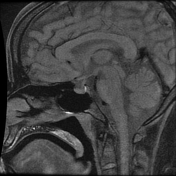
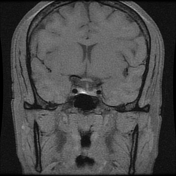
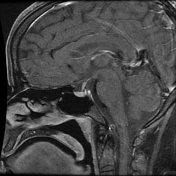
Hypothalamic pituitary axis:
The anterior pituitary is normal in size, shape, morphology, and signal intensity. It measures 6mm x 10mm x 15mm (CC/APTR). On the post-contrast dynamic study, no abnormal lesion is seen in the anterior pituitary.
The infundibular stalk is central in position and normal in thickness.
Posterior pituitary bright spot is orthotopic in position.
The pituitary fossa, the cavernous sinus, bilateral internal carotid arteries (and its branches), and the basilar artery are unremarkable.
Case Discussion
Normal MRI brain and hypothalamic-pituitary axis with incidental finding of right maxillary sinusitis.
A typical upper level of normal is ~40 ng/mL (equivalent to ~850 mIU/L).
Elevated prolactin can be due to a number of causes, including elevated production/secretion as well as reduced inhibition.
Causes are pituitary stalk effect, Medication such as dopamine antagonist, prolactin-secreting tumour.
In this case, the patient was taking a drug called PAN-D 40 (combination pantoprazole and domperidone) for gastritis. The use of a D2 blocker (domperidone) may be the possible cause of the increased serum prolactin level.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.