
Post intubation tracheal injury with pneumomediastinum, pneumothorax and massive subcutaneous emphysema
Presentation
Comatose patient with high ventilator parameters.
Patient Data
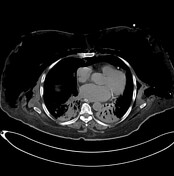

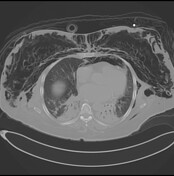


Interruption of the right tracheal wall with loss of its integrity is noted nearly about 3 cm above the carina. Above this level, the tracheal lumen appeases abnormally distended with air. Findings are suggestive of post-intubation tracheal wall injury (PITI) and tear. Intercostal chest tube noted, introduced through the left side of the lateral chest wall, with its end located in the posterior pleural space opposite to the posterior segment of the left upper lobe. Moderate pneumo-mediastinum, mild left-side pneumothorax and pneumomediastinum. Severe extensive bilateral subcutaneous and inter-muscular planes surgical emphysema was noted involving the anterior, lateral, and posterior chest wall, extending to the neck. Bilateral lower lobes consolidations as described, likely of infectious etiology.
Case Discussion
Orotracheal intubation is a routine and common procedure that has potential complications such as tracheal wall injury which is rare but has serious consequences such as pneumomediastinum, pneumothorax and massive subcutaneous emphysema. It was estimated that the incidence of post-intubation tracheal injury is 1 in 20,000 intubations.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.