
Presentation
Headache, a mental disorder with disorientation and agitation in the postpartum period (puerperal).
Patient Data


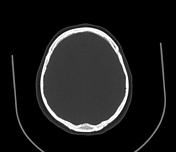

Computed tomography (CT) shows the brain parenchyma is preserved, with no intracranial haemorrhage or ischaemic lesions. The ventricular system and cisternal spaces appear normal. The visualised orbits, paranasal sinuses, and calvaria appear unremarkable.
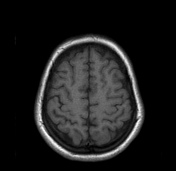
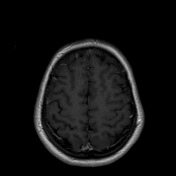
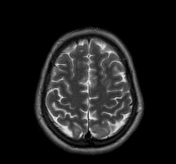
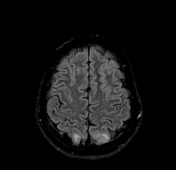

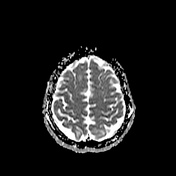
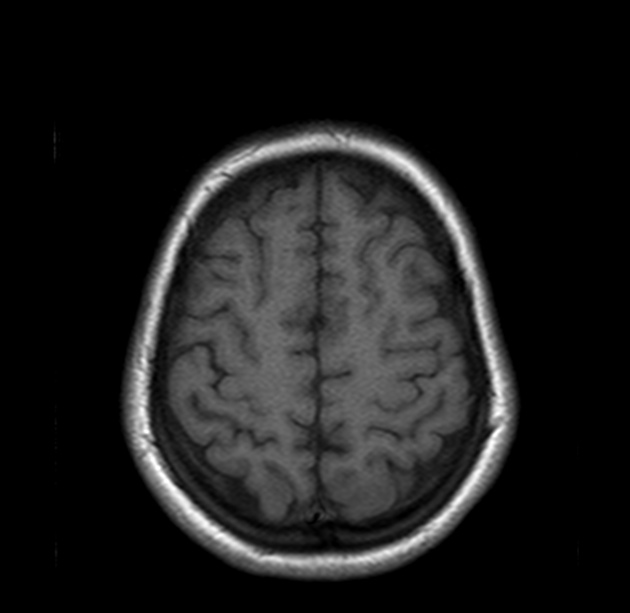
Magnetic resonance imaging (MRI) demonstrates the bilateral cortex and subcortical white matter T2/Fluid-attenuated inversion recovery (FLAIR) hyperintensities in the posterior parietal lobes, which correspond to vasogenic oedema, suggestive of PRES. The oedema distribution is in the posterior cerebral artery (PCA) regions. MR diffusion-weighted imaging (DWI) confirms that the area of abnormality represents vasogenic oedema, without restricted diffusion.
Case Discussion
Posterior reversible encephalopathy syndrome (PRES) is a clinical-radiological syndrome associated with some complex conditions such as preeclampsia/eclampsia, autoimmune disease, high dose cancer chemotherapy, after allogeneic bone marrow transplantation, solid organ transplantation, renal failure, and hypertension 1-5.
This syndrome manifests by a headache, altered mental status, seizures, and visual loss 1,3,4. It is commonly, but not always associated with acute hypertension. A potentially reversible imaging pattern accompanies the disease 4.
PRES can have a variety of imaging findings on CT, MRI, and angiography 4. The typical findings are symmetric vasogenic oedema affecting the parietooccipital cortex and subcortical white matter 1,3. PRES sometimes extend from the posterior to other parts of the brain such as the frontal and temporal lobes, basal ganglia, brain stem, and cerebellum. Lesion confluence may develop as the extent of oedema increases 1.
Atypically unilateral or asymmetrical distribution of oedema in PRES can occur 4,5. Besides, it may progress to atypical appearances including haemorrhage, contrast enhancement, or diffusion-weighted restriction 1,5.
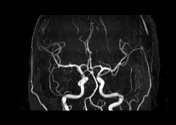
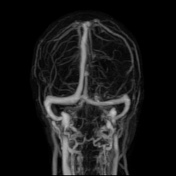
Focal areas of restricted diffusion, similar to infarction or tissue damage with cytotoxic oedema are uncommon 1. Atypical imaging findings should not dissuade the diagnosis of PRES in the appropriate clinical situation 4. Vasculopathy may be identified by CA or MRA.
Case courtesy
- Erick Cavalcante, MD - PGY-3, Radiology Resident, Department of Radiology
- Antonio Rodrigues de Aguiar Neto, MD - Radiologist, Department of Radiology
- Hospital da Restauração – Recife, PE – Brazil


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.