
Presentation
Presented with seizures for 1 day. High blood pressure - 190/110. H/o normal vaginal delivery 3 months back. The patient also complained of swelling of both legs up to knee for 20 days, associated with abdominal distention and facial puffiness. Not a known hypertensive or diabetic. No history of previous epilepsy, TB, bronchial asthma.
Patient Data
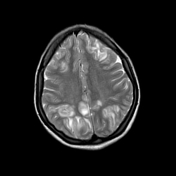

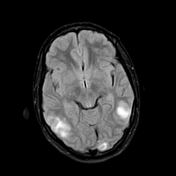
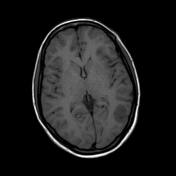
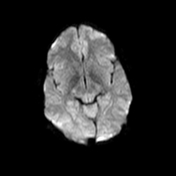
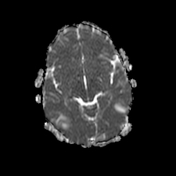
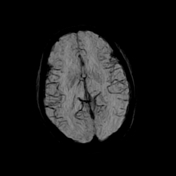
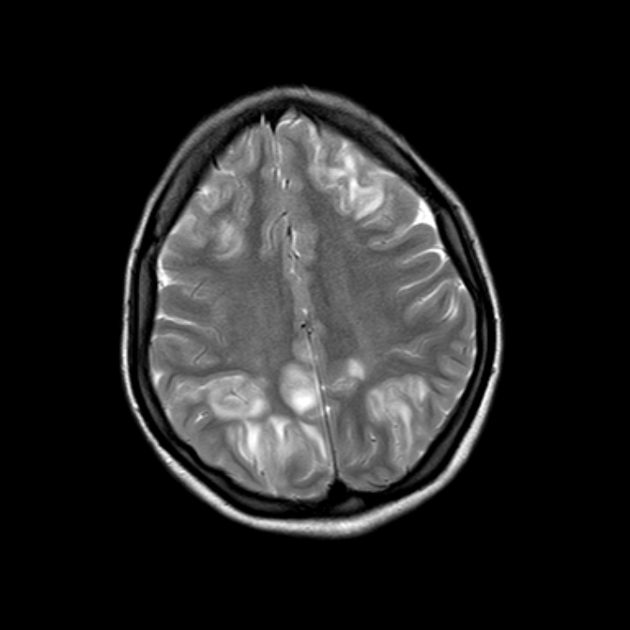
T1 isointense T2/FLAIR hyperintense symmetrical cortical and subcortical foci noted in bilateral frontal, parietal, occipital and inferior temporal regions. No diffusion restriction seen.
Rest of the cerebral hemispheres show normal grey-white differentiation and signal intensity.
Features are suggestive of atypical PRES.
Case Discussion
Posterior reversible encephalopathy syndrome (PRES) also called acute hypertensive encephalopathy and reversible posterior leukoencephalopathy syndrome (RPLS).
Aetiologies include preeclampsia/eclampsia, bone marrow/organ transplantation, autoimmune diseases, high dose chemotherapy, etc.
Imaging findings - symmetrical cortical and subcortical hyperintense signals on T2/FLAIR images in the parieto-occipital lobes of both cerebral hemispheres. Imaging findings may vary and can occur in any location. Diffusion restriction and haemorrhage are rare but can occur.
It is a disorder of cerebrovascular autoregulation.
Differential diagnosis includes cerebral infarction, cerebral venous thrombosis, hypoxic brain damage, hypoglycaemic brain injury, and encephalitis. PRES is usually reversible, but permanent damage can occur if cerebral ischaemia or haemorrhage occurs.
Treatment is targeted to the precipitating cause - such as blood pressure management in this case.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.