
Presentation
Progressive history of left sided epiphoria, worsening proptosis and declining vision. Optic nerve swelling and ophthalmoplegia on examination.
Patient Data




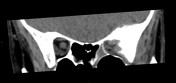

Spiculated lesion centred in left greater wing of sphenoid and lateral orbital wall. Cortical erosion, with soft tissue and periosteal new bone formation. Optic canal not involved. Extension into middle cranial fossa but no gross underlying brain change.
Similar appearance in left occipital bone.
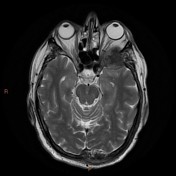
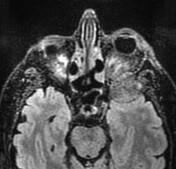
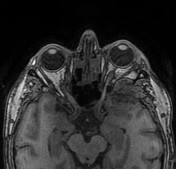
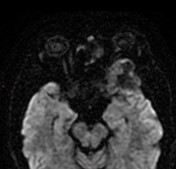
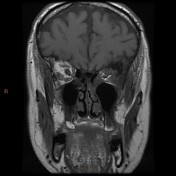
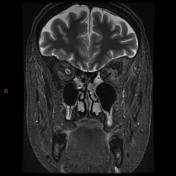
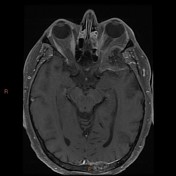
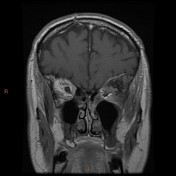
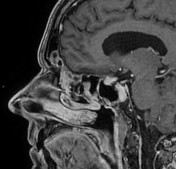
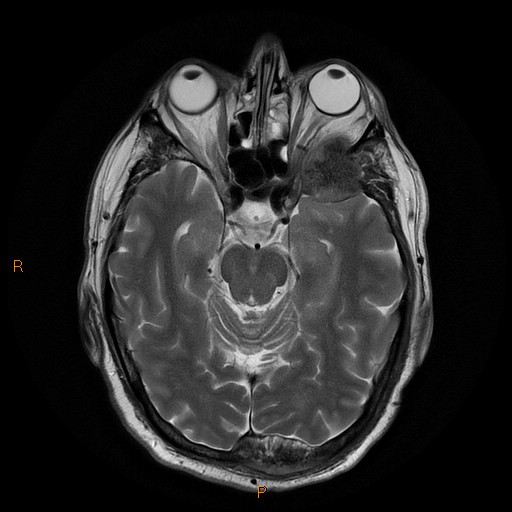
As on CT, tumour deposit in left lateral orbital wall, approximately 4 cm. Irregular spiculated sclerotic centre. Enhancing soft tissue components, and of the adjacent dura. Abutment of the pterygopalatine fossa but no direct extension. No abnormal enhancement of the maxillary trigeminal division or cavernous sinus.
Displaced lateral rectus muscle and inseparable but likely displaced superior rectus muscle. Distorted optic nerve with effacement of the optic sheathe but normal nerve signal at the orbital apex.
Similar characteristics in left occipital bone, and further possible lesion in right mandible.
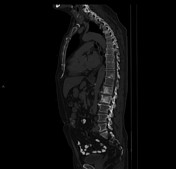
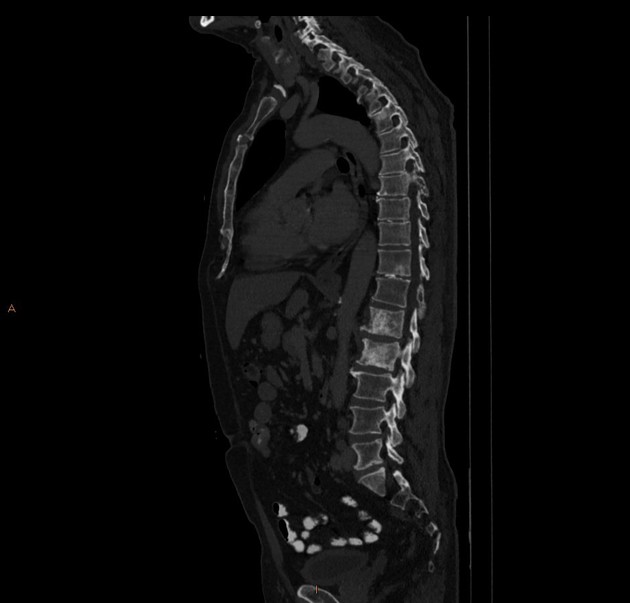
Multiple mixed lytic and sclerotic skeletal metastases; no imminent spinal canal compromise.
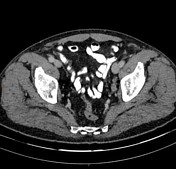
Iliac and para-aortic pathological nodal enlargement.
Case Discussion
PSA was confirmed at over 1800 ug/L, with imaging features compatible with metastatic prostate cancer.
This was managed with chemotherapy and hormone injections with good clinical response and reduced size of skull metastases on follow-up imaging.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.