
Presentation
Acute severe headache.
Patient Data


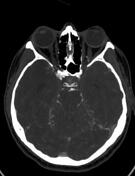



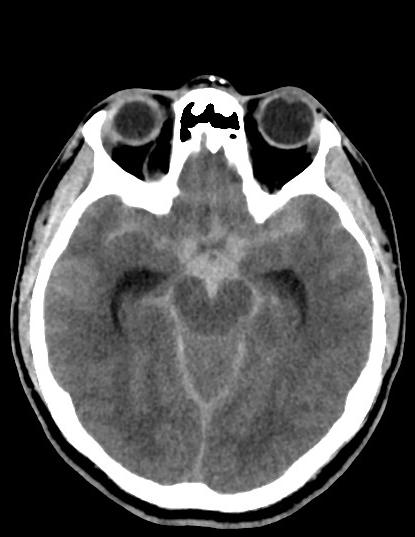
Non-contrast CT head
extensive bilateral subarachnoid hemorrhage - perimesencephalic; in all the basal cisterns; in the narrowed third ventricle, Sylvian aqueduct, and fourth ventricle; in the premedullary cistern; in the Sylvian cisterns and fissures; in the interhemispheric fissure; and bifrontal
the temporal horns of the lateral ventricles are dilated - early sign of hydrocephalus
the cerebral and cerebellar sulci are effaced - suggestive of brain edema
CT angiogram
pedunculated aneurysm with a "nipple" at the basilar tip measuring 3 mm in diameter and 5.5 mm in length, deviating to the left P1
the intracranial arteries appear slightly narrowed, perhaps due to cerebral edema
the neck arteries are patent
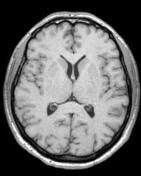
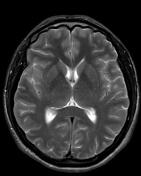
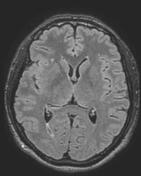
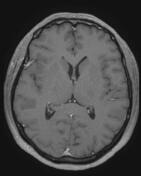
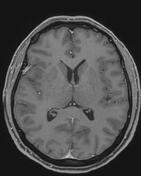
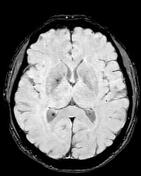
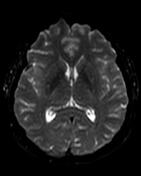
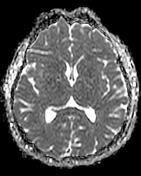
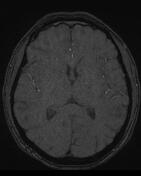
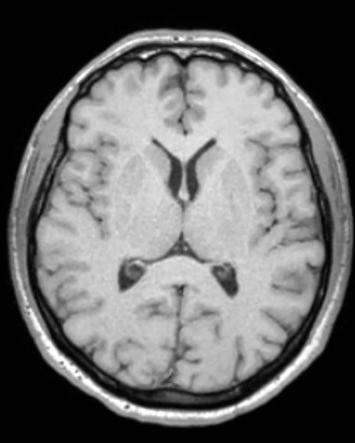
3-month follow-up MRI:
MRA: filling defect between basilar tip and left PCA, representing the embolization coils in the aneurysm
no evidence of new aneurysm
SWI: blood degradation products on the tentorial leaflets and in the basal cisterns, as well as small amount mainly in the biparietal sulci and bifrontal sulci around the vertex
two tiny foci of susceptibility artifact in the right cerebellar hemisphere and one in the left hemisphere
above the tentorium: several nonspecific abnormal white matter foci on the right, single one on the left - probably representing microangiopathy
no abnormal port-contrast enhancement
Case Discussion
An otherwise healthy woman complained of a severe headache that started that same morning. Blood pressure taken at the ED was 210 mmHg systolic. She was sent for a CT head-CTA neck and head arteries, for fear that a subarachnoid hemorrhage was the cause of her headache.
CT head showed extensive subarachnoid bleeding, as well as signs of brain edema and mild hydrocephalus, while the CTA revealed a small basilar tip aneurysm.
The aneurysm was successfully coiled, and the patient recovered promptly and uneventfully.
An MRI head done 3 months later showed only subtle hemosiderin deposits on SWI.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.