
Presentation
Nasal obstruction and headache. History of previous surgery for recurrent sinonasal polyposis.
Patient Data
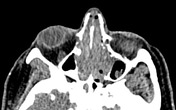

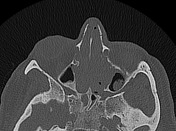
Partial opacification of both maxillary and sphenoid sinuses and near total opacification of both frontal sinuses and ethmoid air cells with soft tissue density contents, mucosal thickening, retained secretions and retention cysts. Rarefaction of ethmoid bony septae, nasal turbinates and upper part of bony nasal septum are also noted. Mucosal obstruction, widening and remodeling of the ostiomeatal complexes and sphenoethmoidal recesses.
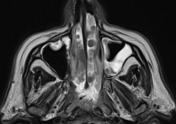
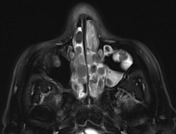
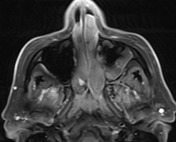


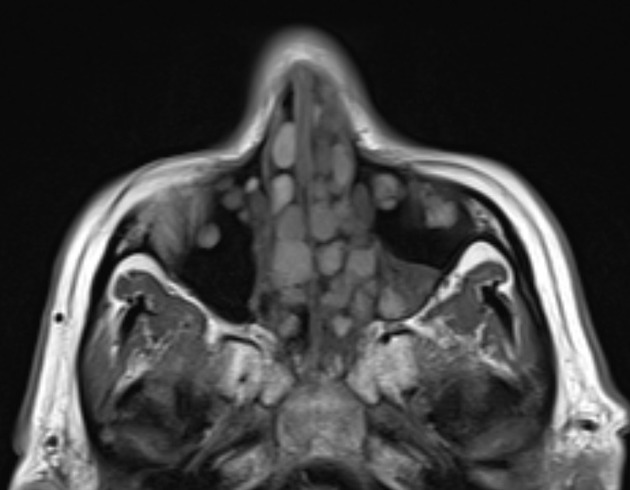
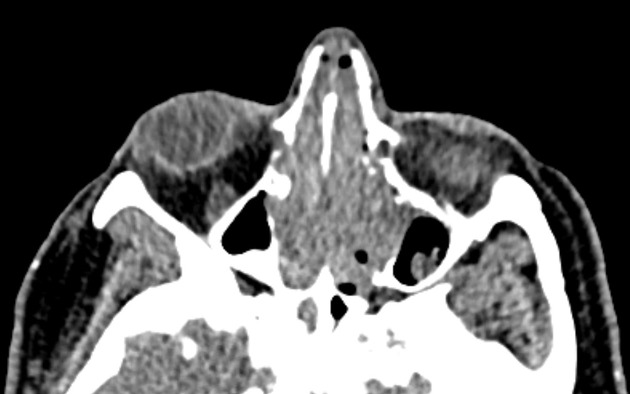
Opacification of all paranasal sinuses, nasal cavity and ethmoidal air cells bilaterally by polypoid mucosal thickening and retained secretions.
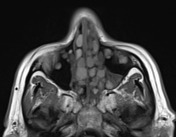
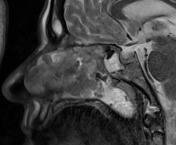
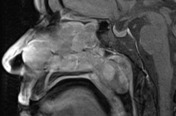
Numerous sinonasal polyps are noted with intermediate to high signals on T1 and intermediate to low signal intensity on T2 are noted with smooth outline. A nasopharyngeal polypoidal extension is noted compromising airway is noted. Following gadolinium, thin linear mucosal enhancement is noted, the polyps are non-enhancing. No suspicious masses.
No sinus walls bony erosions. Clear peri-antral fat planes. Intact skull base and lamina papyracea. No intra-cranial or orbital extensions.
Incidentally noted left sphenoid ridge wide dural-based lesion with intense homogeneous enhancement denoting left sphenoid ridge meningioma.
Case Discussion
Features are suggestive of benign sinonasal polyposis on top of chronic sinusitis. Contrast-enhanced MRI helps to differentiate it from probable malignant sinonasal tumors.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.