
Presentation
Two days of dysarthria, right facial numbness, right facial drooping, and right ear pressure.
Patient Data
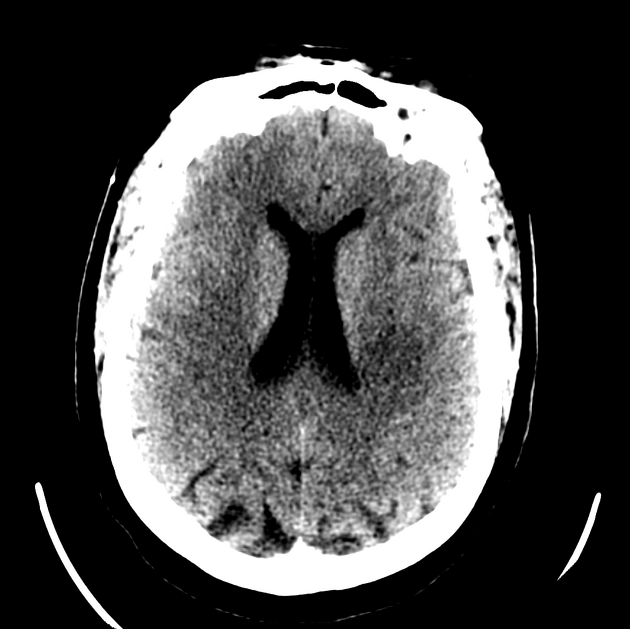
The initial computed tomography scan (CT) showed subtle hypodensity in the left capsule and frontoparietal white matter.
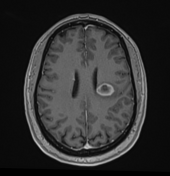

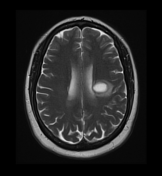
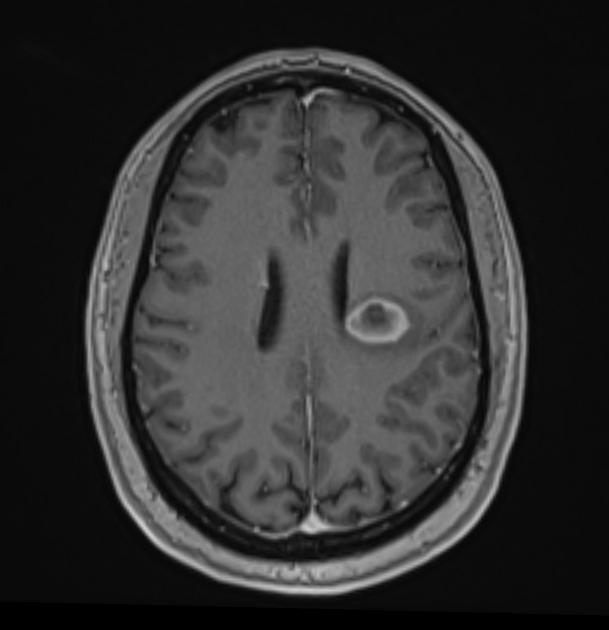
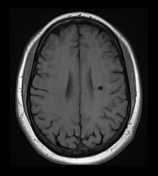
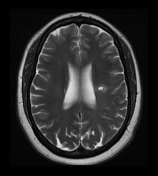
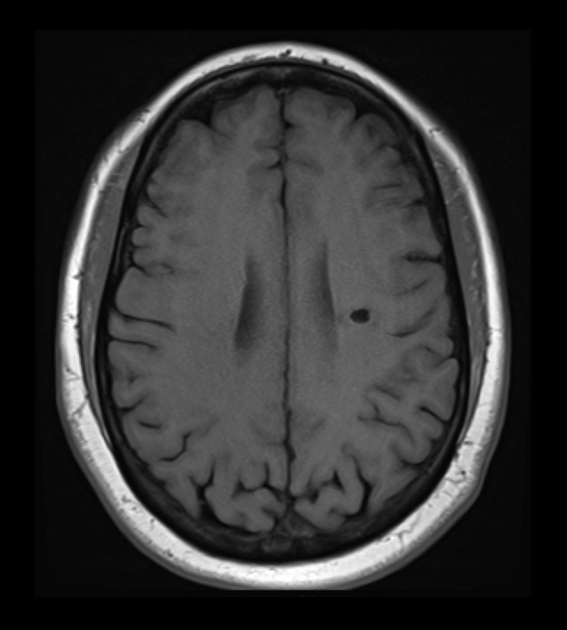
A well-defined high T2 signal lesion with a hypointense rim, surrounded by oedema in the left corona radiata, abuts the lateral ventricle. It has prominent peripheral contrast enhancement completely encircling the lesion. The periphery (enhancing) component demonstrated some diffusion restriction but the central component did not (not shown).
On the right, at a similar location, is a non-specific small area of high T2 signal. Otherwise, no other lesions are identified.
The patient underwent a lumbar puncture and needle biopsy of the lesion.
Histology
Biopsies revealed glial tissue containing sheets of macrophages and focal perivascular mild chronic inflammation. Immunostains indicated the cells lacked glial fibrillary acidic protein (GFAP) expression, while fragmented glial fibres were prominently displayed. CD68 highlighted the macrophage sheets, while CD3 marked lymphocytes surrounding the perivascular region. PAX-5 staining revealed B lymphocytes scattered in the perivascular area, while CD138 highlighted plasma cells. Staining for Epstein-Barr virus and microorganisms was negative. Additional staining showed intact neurofilaments, polytypic plasma cells, and a loss of myelin.
Overall, the pathology results aligned with a demyelinating process.
The patient was subsequently prescribed Natalizumab, a standard treatment for MS 1.
The previously observed enhancing circular lesion in the left centrum semiovale markedly decreased in size. No other new lesions.
Case Discussion
Brain MRI scans for this lesion appeared as hyperintense signals on T2-weighted imaging and hypointense signals on T1-weighted imaging, which is typical for a demyelinating process 2. Specifically, hypointensity in T1-weighed imaging and hyperintensities in T2-weighted imaging are consistent with solitary demyelinating lesions 3. Furthermore, solitary demyelinating lesions are commonly located in the white matter, specifically in the periventricular areas 4, seen in the MRI scans. Demyelinating lesions show a contrast enhancement pattern that appears to be an open ring with relatively little mass effect or surrounding oedema 5. A defining factor of solitary tumefactive demyelinating lesions is their large size, typically greater than 2 cm. In contrast, the lesion was 1.9 cm, similar to other cases involving solitary tumefactive demyelinating lesions.
The expression of CD68 indicates macrophage infiltration in affected tissues of demyelinating diseases 7. It can highlight the presence of foamy macrophages within the demyelinated areas, which are a feature of solitary demyelinating lesions 8. The presence of CD68 can indicate accumulation of macrophages, suggesting an ongoing inflammatory process typical of demyelination. Furthermore, the presence of fragmented glial fibres from the absence of GFAP has been observed in the demyelinated lesions. CD138-expressing plasma cells may be a contributing factor to the inflammatory response. It may not be a primary marker for solitary demyelinating lesions. However, it could be expressed by reactive plasma cells within the lesion 9. Another biomarker, CD3, is regularly used to identify lymphocytes, specifically T cells, which are a type of white blood cell involved in an immune response 10. In demyelinating diseases, lymphocytes are known to accumulate around blood vessels in the CNS and are also a feature of inflammatory lesions 11. This inflammatory process is a crucial sign of solitary demyelinating lesions 12.
Balo concentric sclerosis is a rare subtype of multiple sclerosis that appears as a rounded lesion with alternating high and low signal intensity on MRI 13. It has a characteristic ‘bullseye’ or ‘onion bulb’ appearance. Based solely on the MRI scans, the open-ring pattern in this case would make it a solitary demyelinating lesion (tumefactive demyelination) rather than Balo concentric sclerosis.
Additional Contributors:


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.