
Presentation
Abdominal pains with six months amenorrhoea, on implanon.
Patient Data

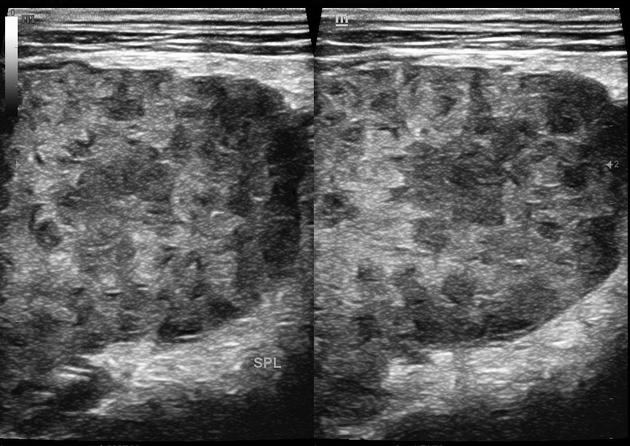
Diffuse multiple hypoechoic wedge-shaped defects are littered within the entire splenic parenchymal surface that minimally geographically spares island areas of normal splenic parenchyma. There is resultant mild splenic enlargement (current splenic index = 78.1 cm2). Colour Doppler imaging reveals insignificant vascularity within the lesions. The rest of the abdominal-pelvic structures grossly looked normal.
Case Discussion
A near miss (with a curvilinear probe) splenetic anomaly during abdominal sonography. Notice how insignificant the tiny lesions almost appear on a curvilinear sector probe, albeit with a change in technique to a high resolution linear sector array transducer, conspicuously pronounces the lesions now unmistakably. No gross abdominal-pelvic lymphadenopathy identified.
In the setting of such heterogenous and multifocal splenic parenchymal lesions, plausible differentials to consider may include 1-7:
splenic tuberculosis (hypoechoic small multiple lesions within the splenic parenchyma, likely microabscesses, as in the case above where the patient is being managed for disseminated pulmonary tuberculosis, is on ARV/HIV drugs and is on management for acute kidney infection. The PTB was confirmed with a positive LAM test on a follow-up.
multiple splenic infarcts (hypoechoic variable-sized lesions, permeating and void of target appearance)
lymphoproliferative splenic disorder (may present with target appearance and with para-aortic/retroperitoneal lymphadenopathy)
sarcoidosis (extensive/massive splenomegaly; diffusely heterogenous)
Hodgkin's disease and malignant lymphoma [mostly target lesion(s). Should be further supported clinically and/ or with other imaging modalities]
other haematological disorders


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.