
Presentation
1-day history of shoulder pain following physical therapy.
Patient Data


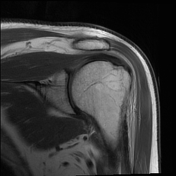
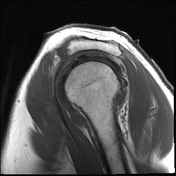

Moderate subdeltoid bursitis. Type III acromial pathology. Correlate clinically for symptomatic subacromial shoulder impingement.
The teres minor is intact. There is insertional infraspinatus tendinosis without tears. There is insertional supraspinatus tendinosis with a 0.6 x 0.3 cm partial-thickness interstitial tendon tear at the footprint. There is mild subscapularis tendinosis without a tear. The long biceps tendon is maintained in an anatomical location without tear.
There is no acute Hill-Sachs or Bankart lesion. There is a tear of the anterosuperior, superior, and posterosuperior labrums, reflecting a SLAP lesion.
The articular cartilage of the humeral head and glenoid appears intact.
Suprascapular and spinoglenoid notches, as well as those that follow, have preserved the surrounding fat planes. There is no evidence of muscle atrophy or denervation edema. Mild edema of the anterior and lateral bellies of the deltoid suggests myositis or strain.
Case Discussion
Shoulder impingement (SI) is a common cause of shoulder pain. SI is more prevalent among people who engage in overhead movements, including swimming, painting, throwing, gymnastics, and stocking shelves. In our case, the patient presented with acute, exacerbated shoulder pain following a physical therapy session. A diagnosis was confirmed via MRI, and he was treated with rest and NSAIDs.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.