
Presentation
Headache, dizziness and vertigo
Patient Data
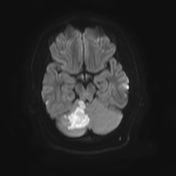

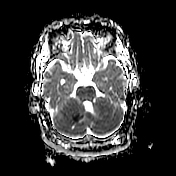
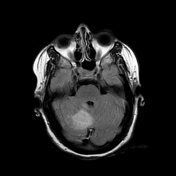
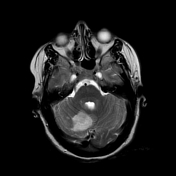
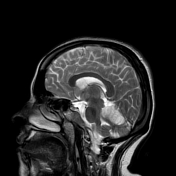
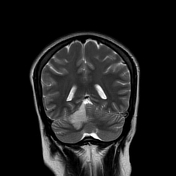
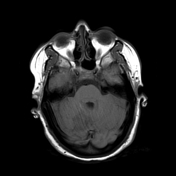
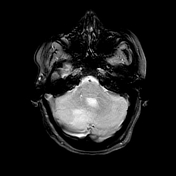
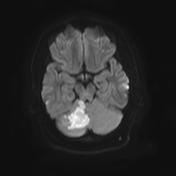
There is a geographic hypointense T1 and hyperintense T2/FLAIR lesion in the superomedial aspect of the right cerebellar hemisphere with partial involvement of the superior vermis. It showed diffusion restriction on DWI/ADC map.
No involvement of the midbrain. No intracerebral haemorrhage or extra-axial haematoma. No masses. No hydrocephalus.
Case Discussion
Appearances, in this case, are compatible with an acute right distal superior cerebellar artery infarction. It accounts for about 50% of cerebellar infarcts. Two patterns are described according to the site of occlusion:
- occlusion at the origin of the artery results in cerebellar and brain stem signs with contralateral sensory impairment
- peripheral occlusion results in ipsilateral cerebellar signs as in this case
Causes include atherosclerosis, emboli and dissection of vertebral or basilar arteries. This case is likely due to embolic cause.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.