
Presentation
4 weeks of falls and dizziness. Background of HTN, hypercholesterolemia and previous traumatic brain injury. Neurologically intact on examination.
Patient Data
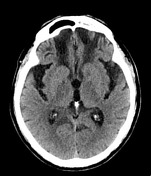

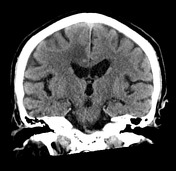

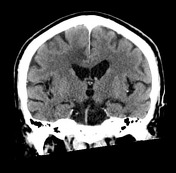

Multilobulated ring enhancing lesion in the posterior medial right frontal lobe. Marked surrounding vasogenic edema. Bifrontal areas of encephalomalacia in keeping with previous traumatic brain injury.
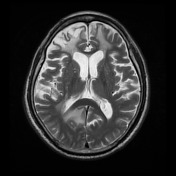
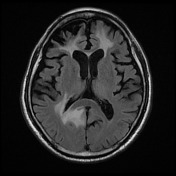
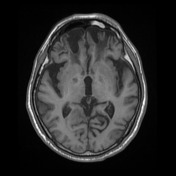
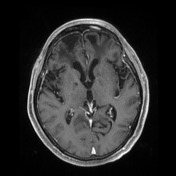
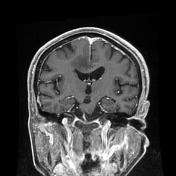
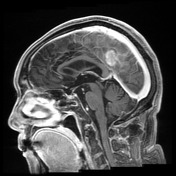
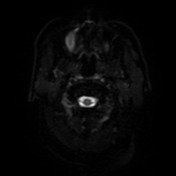
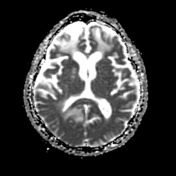
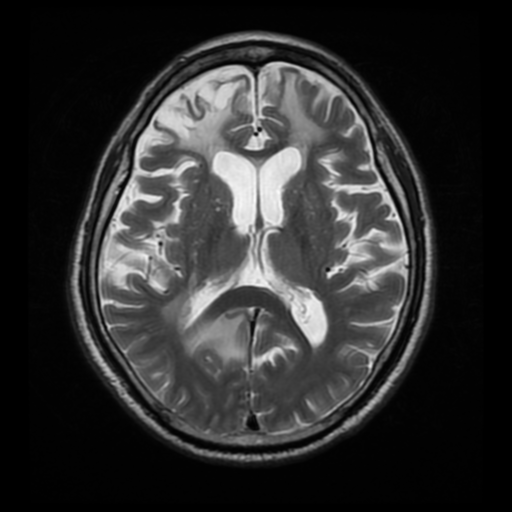
Multilobulated ring enhancing lesion in the posterior medial right frontal lobe with marked surrounding vasogenic edema. Mild central restricted diffusion. The dural venous sinuses are patent. Bilateral frontal encephalomalacia in keeping with previous traumatic brain injury.
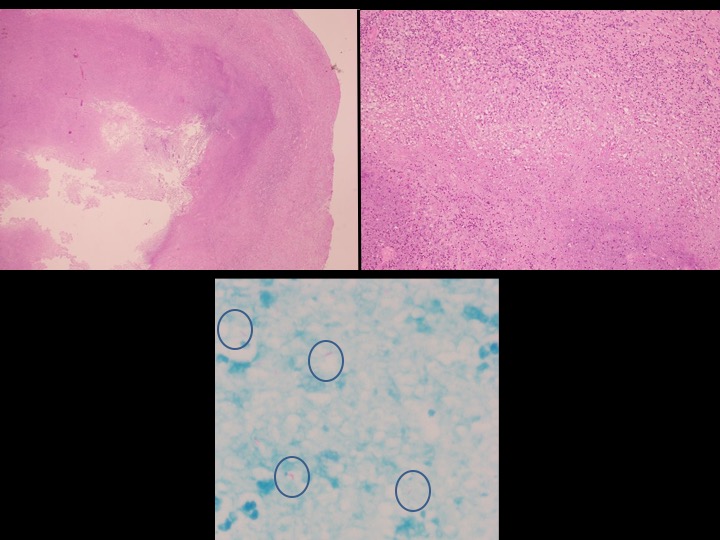
Histopathology: The sections show a cerebral abscess. The contents comprise necrotic inflammatory debris. This is delimited by a layer of inflamed vascular granulation tissue. There is an encompassing mantle of edematous and gliotic brain parenchyma in which there are multiple foci of active cerebritis. There is no evidence of tumor. Numerous acid-fast bacilli with beaded morphology are identified in a Ziehl-Neelsen stained section.
DIAGNOSIS: Tuberculous cerebral abscess.
Case Discussion
In the brain, tuberculosis can cause tuberculous meningitis, tuberculomas or tuberculous abscess. A tuberculous abscess has a capsule containing pus and acid-fast bacilli. It is similar to a pyogenic abscess. Tuberculomas, on the other hand, do not contain pus; however, they may contain necrotic material. Intracranial tuberculomas are usually an extension of meningitis and are usually multiple, while tuberculous abscess, as in this case, is usually solitary.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.