
Presentation
Presented to GP with haematuria. Abdominal examination demonstrated a large right upper quadrant mass.
Patient Data
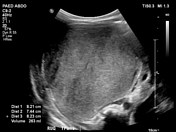




8.2 cm mass in the right upper quadrant with internal vascularity, appearing to arise the superior pole of the right kidney. Findings concerning for a neoplastic process with no evidence of renal vein or inferior vena cava tumour thrombus.
Left kidney appears normal.

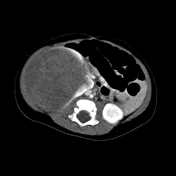


CT demonstrates a large, expansile retroperitoneal mass occupying a large portion of the right hemi-abdomen, demonstrating a claw sign with the renal parenchymal confirming renal origin.
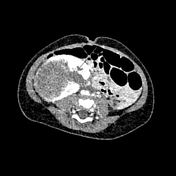
The lesion is predominantly hypodense with interspersed hyperdense areas within . At its infero-medial aspect, the lesion appears to extend into the renal pelvis. The inferior pole of the right kidney demonstrates a mild degree of hydronephrosis although the parenchyma itself has a normal appearance.
Small volume, presumably reactive hypodense fluid is noted in the right paracolic gutter.
Subcentimetre pre and paraaortic lymph nodes of equivocal significance.
HISTOLOGY
Nephroblastoma (Wilms tumour). The tumour consists predominantly of stroma (60%) with areas of skeletal muscle differentiation. Scattered through the stroma are areas of blastema (30%) some of which are associated with tubule formation (10%). There is no evidence of anaplasia. Necrosis is present. The tumour infiltrates into the renal hilar adipose tissue but does not involve the venous or lymphatic vascular spaces.
Case Discussion
Wilms tumours are the most common paediatric renal tumours. Median age at diagnostic is 3.
The most common presentation is of a painless upper abdominal mass.
This case demonstrates a good example of the claw sign, indicating that the mass originates from the kidney.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.