
Acute calcific periarthritis is an acutely painful monoarticular condition characterised by the juxta-articular deposition of calcium hydroxyapatite crystals and local inflammation.
On this page:
Epidemiology
Affects both males and females over a wide age range, however, occurs more frequently in females than males between the ages of 40 to 70 years.
Clinical presentation
sudden onset of severe pain and swelling around one joint, usually of finger or toe
no history of acute trauma
no fever, systemic complaints or arthralgia of other joints
Pathology
Acute juxta-articular soft tissue deposition of calcium hydroxyapatite crystals leads to an acute inflammatory response.
Types
Acute calcific periarthritis is thought to represent a clinical subset of hydroxyapatite deposition disease (HADD) and occurs when crystals are acutely deposited in the periarticular capsular structures:
HADD in tendons results in calcific tendonitis
HADD in bursa results in calcific bursitis
HADD in shoulder joint results in Milwaukee shoulder
Radiographic features
Plain radiograph
Well-circumscribed ovoid or curvilinear calcification adjacent to a joint (usually on one side).
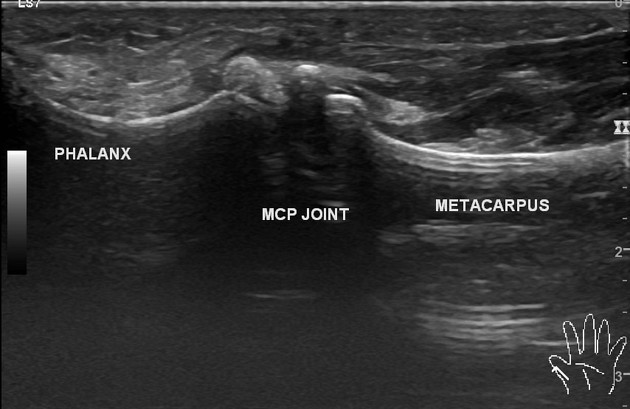
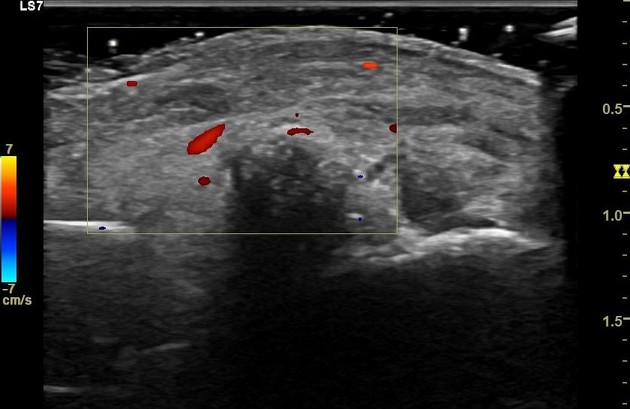
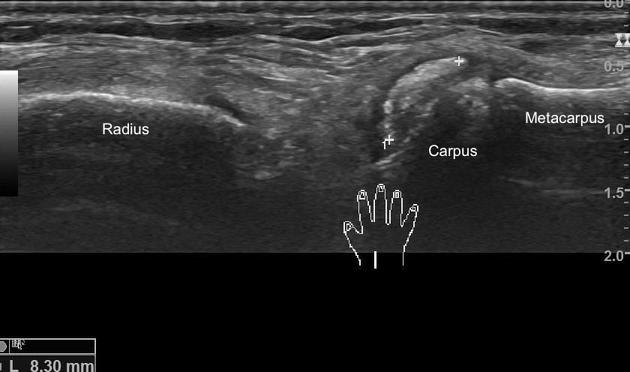
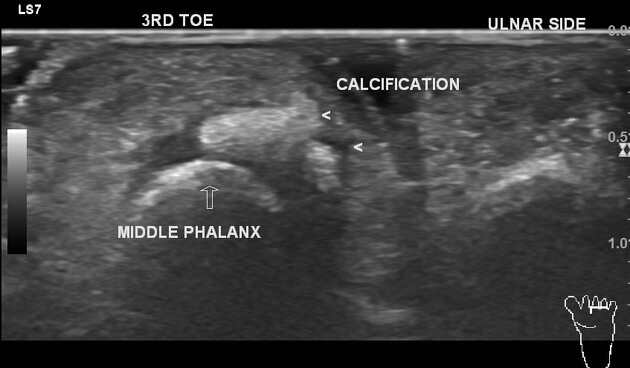
Ultrasound
curvilinear/ovoid calcification with acoustic shadowing
capsular soft tissue swelling
CT
periarticular calcification
MRI
generally low signal from calcification
high signal on fluid weighted sequences from soft tissue oedema
Treatment and prognosis
managed conservatively with nonsteroidal anti-inflammatory drugs
may require corticosteroid injection
usually responds to treatment within a week with resolution of the acute symptoms
periarticular calcification significantly decreases in 3-4 weeks but takes longer to clear, typically 6-8 weeks
Differential diagnosis
infectious arthritis (soft tissue calcification is not seen in acute septic arthritis)
tendon-related HADD
Other causes of soft tissue calcification such as:
Practical points
acute calcific periarthritis should be considered when faced with an acutely painful finger, especially in the presence of periarticular calcification on radiographs or ultrasound
recognising the clinical presentation with correlation of imaging would avoid unnecessary treatments such as antibiotics or surgery




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.