
Primary adenocarcinoma of the small bowel is about 50 times less common than colon adenocarcinoma.
On this page:
Epidemiology
Risk factors
Risk factors include a history of ref:
congenital bowel duplication
ileostomy, or duodenal or jejunal bypass surgery
Pathology
Almost 50% of small bowel adenocarcinomas are found in the duodenum, especially near the ampulla. In the remaining cases, the jejunum is more commonly involved than the ileum 1.
More distal small bowel adenocarcinomas are more likely to be annular, duodenal adenocarcinomas tend to be papillary or polyploid 1.
Radiographic features
CT
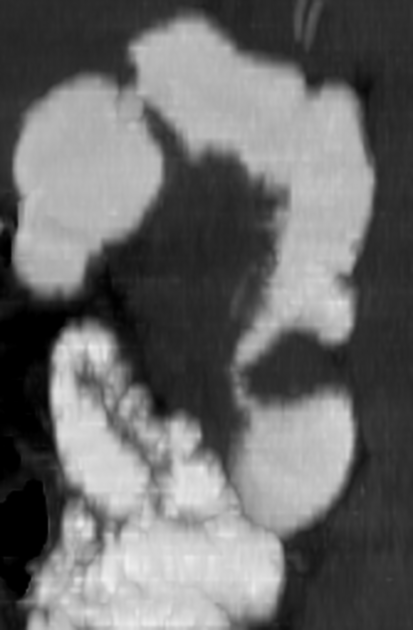
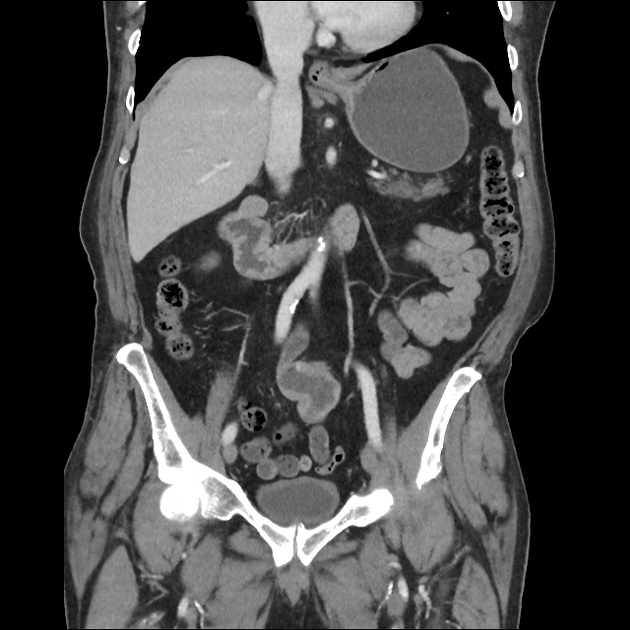
CT shows a soft-tissue mass with heterogeneous attenuation, usually with moderate enhancement after intravenous administration of contrast material.
The mass may manifest as an annular narrowing with abrupt concentric or irregular “overhanging edges”, a discrete tumor mass or an ulcerative lesion.
Usually, only a short segment of the bowel is involved. Gradual narrowing of the lumen leads to partial or complete small bowel obstruction 1.
A large, aggressive, ulcerated adenocarcinoma can be mistaken for lymphoma. However, lymph node metastases in adenocarcinoma are usually less bulky than those in lymphoma.
Differential diagnosis
Small bowel malignant tumors:
leiomyosarcoma
malignant GIST
Small bowel benign tumors:
adenomatous polyp
villous adenoma
leiomyoma
lipoma
hamartoma
hemangioma








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.