
Amnestic syndrome of the subcallosal artery describes an acute amnestic syndrome secondary to ischaemic stroke affecting the subcallosal artery, which leads to infarction of the bilateral fornices.
On this page:
Epidemiology
The incidence of amnestic syndrome of the subcallosal artery is unknown, but it is likely to be very rare ref.
Clinical presentation
The typical clinical presentation is that of acute and severe anterograde amnesia, with particular impairment of episodic, rather than semantic, memory 1,2.
Pathology
Amnestic syndrome of the subcallosal artery is caused by infarction in the territory of the subcallosal artery 1-5. The subcallosal artery is a branch from the anterior communicating artery, and infarction of its territory typically results in bilateral forniceal infarction, particularly involving the bilateral columns. However, nearby structures may also be affected 1-5.
The fornices are part of the Papez circuit, which has a key role in memory storage 2. Thus, infarction of the fornices disrupts this circuit, leading to amnesia, which characterises the clinical presentation of amnestic syndrome of the subcallosal artery 2.
Ischaemic stroke of the subcallosal artery can be caused by the typical mechanisms of ischaemic stroke (e.g. thrombotic, cardioembolic), but also iatrogenically after certain neurosurgical interventions (e.g. surgical trapping of anterior communicating artery aneurysms) 1-5.
Radiographic features
MRI
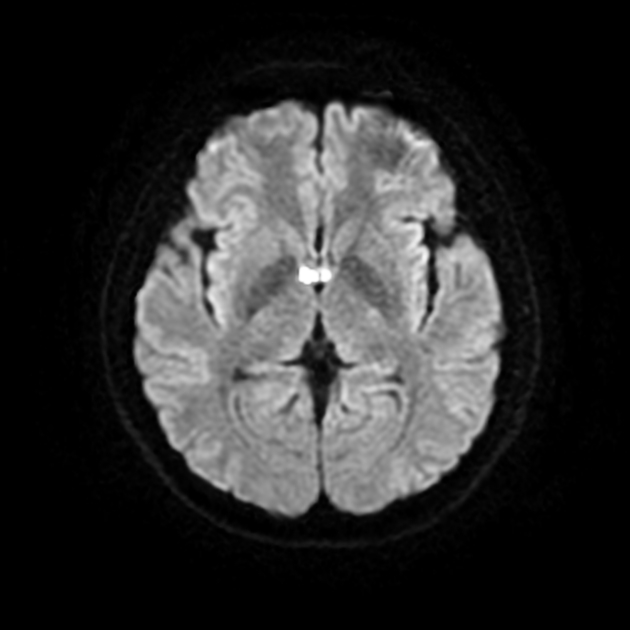
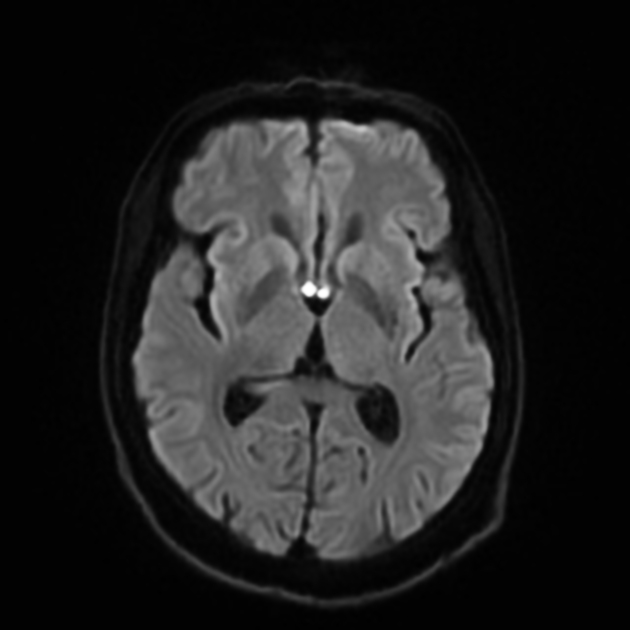
MRI brain is the imaging investigation of choice, and reveals ischaemic stroke in the territory of the subcallosal artery, affecting the bilateral fornices and other nearby structures such as the anterior corpus callosum, septal nuclei, and septum pellucidum 1,2,5. See ischaemic stroke for a detailed description of the expected MRI findings.
A number of radiological signs have been proposed to describe the appearance of high signal on axial DWI affecting the bilateral fornices and genu of the corpus callosum 2:
'goblet sign': describing the appearance of a goblet 5
'watch out sign' or 'warning sign': describing the appearance of an exclamation mark (or exclamation point) 6
MR angiography may reveal occlusion (or a filling defect) of the subcallosal artery, particularly on sagittal views 5, but this may be difficult to visualise given the small calibre of the subcallosal artery.
Treatment and prognosis
Management does not differ from other presentations of ischaemic stroke ref.
History and etymology
Amnestic syndrome of the subcallosal artery was first described in 2005 3, although there were case reports prior to this describing amnesia in the setting of forniceal infarction 7.
Differential diagnosis
Clinical differential diagnoses include:
transient global amnesia, has DWI high signal affecting the CA1 area of the hippocampus
other strategic ischaemic stroke (e.g. hippocampal infarct)
transient epileptic amnesia, typically present upon waking
psychogenic amnesia, more-so affects semantic memory compared to episodic memory
drug-related amnesia, typically has features of encephalopathy
post-traumatic amnesia, has a history of trauma


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.