
Angiocentric gliomas are rare, superficial slow-growing WHO grade 1 brain tumours typically presenting in paediatric patients with intractable focal epilepsy 1-6. They are often considered part of the heterogeneous group of tumours known as long-term epilepsy-associated tumours (LEATs).
On this page:
Epidemiology
Angiocentric gliomas are very rare tumours with relatively few reported cases. They usually affect children and young adults 1,6. No reported gender predilection has been reported 1.
Associations
Cortical dysplasia may be associated.
Clinical presentation
Seizures are the classical presentation, with over 95% of patients presenting with epilepsy 3.
Pathology
Angiocentric gliomas are considered paediatric-type diffuse low-grade gliomas and designated as WHO grade 1 tumour in the WHO brain tumour classification 1-3,7. The exact aetiology of angiocentric gliomas remains unclear although some features are similar to ependymomas 1,6. In fact, sometimes, a distinct ependymoma component may co-exist 1.
Microscopic appearance
These tumours demonstrate a monomorphic population of elongated spindle-shaped bipolar cells with a strikingly perivascular orientation, somewhat reminiscent of perivascular pseudorosettes 1,6. Although tumour cells do extend into the surrounding parenchyma, a strong predilection for perivascular spread is evident 6. Subpial growth along the surface of the cortex is also a prominent feature 1,6.
Immunophenotype
The immunophenotype shares some similarities to ependymomas 1.
Ki-67 index is usually <5% 1.
They do not demonstrate neuronal markers (e.g. synaptophysin, chromogranin-A, neuronal nuclear antigen) and they are isocitrate dehydrogenase (IDH) negative.
Genetics
MYB-QKI gene fusion 8
Radiographic features
Angiocentric gliomas are usually cortical or subcortical (grey-white matter junction), typically well-delineated, supratentorial tumours that tend to expand affected gyri. They exhibit a propensity to spread horizontally in the subpial plane and deeply along vessels 1.
CT
Typically appear as an expansile non-enhancing cortical tumour.
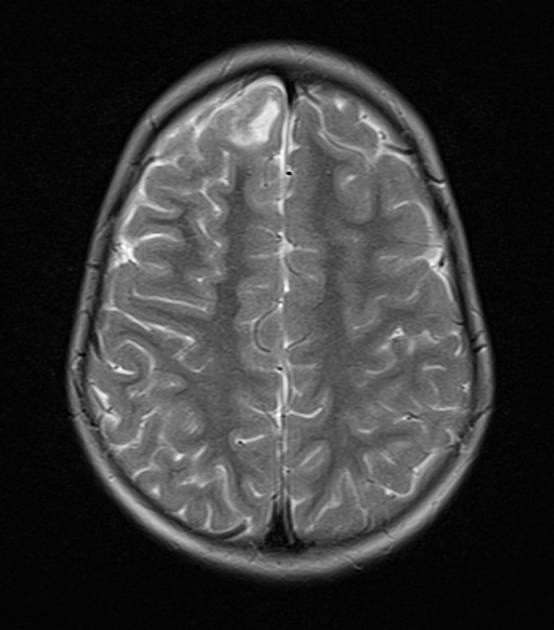
MRI
-
T1
hypointense
hyperintense rim may be seen 4,9
-
T2/FLAIR
hyperintense
extension toward the ventricles along vessels
may have cystic-appearing areas
T1 C+ (Gd): no enhancement
History and etymology
Angiocentric glioma was initially identified in 2005 in two separate case reports 2,5 and then introduced in the WHO classification of CNS tumours in 2007.
Differential diagnosis
Given their rarity, on purely imaging grounds it is difficult to distinguish these tumours from more common diffuse gliomas (both astrocytoma and oligodendroglioma). Other imaging differential considerations include:
cortical tuber (forme fruste of tuberous sclerosis)
-
"bubbly" cortical and subcortical lesion
rim of high signal on FLAIR
minimal surrounding oedema
-
total nulling on the FLAIR sequence
-
usually enhance
well defined
-
multinodular and vacuolating neuronal tumours
subcortical cluster of cystic-like lesions


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.