
Ankle radiographs are frequently performed in emergency departments, usually after trauma. The radiographic series is comprised of three views: an anteroposterior, mortise, and a lateral. They may be performed to assess degenerative or inflammatory arthritis as well as to look for sequelae of local infection.
On this page:
Systematic review
Choosing a search strategy and utilising it consistently is a helpful method to overcome common errors seen in diagnostic radiology. The order in which you interpret the radiograph is a personal preference. A recommended systematic checklist for reviewing musculoskeletal exams is: soft tissue areas, cortical margins, trabecular patterns, bony alignment, joint congruency, and review areas. Review the entire radiograph, regardless of perceived difficulty. Upon identifying an abnormality, do not cease the review, instead put it aside and complete the checklist.
The ring structure of the ankle is made up of three bones (tibia, fibula and talus) and three ligaments (medial and lateral collateral ligaments and interosseous ligament)
if there is one break in the ring, look for a second
Soft tissue
Assess all soft tissue structures for any associated or incidental soft tissue signs such as swelling, stranding, or emphysema.
Ligaments
Like all joints, structural integrity is achieved by the ligaments that hold it together. The ankle has three main sets of ligaments:
medial: deltoid ligament
lateral: posterior talofibular, anterior talofibular and calcaneofibular ligaments
syndesmotic ligament
The deltoid ligament is much stronger than the ligaments that support the lateral aspect of the ankle. This results in a relative difference between the degree of pronation and supination that can be achieved.
Bony anatomy
The ankle is a synovial joint composed of the distal tibia and fibula as they articulate with the talus. The distal tibia and fibula articulate with each other at the distal tibiofibular joint which is more commonly referred to as the tibiofibular syndesmosis (or simply the syndesmosis).
As with all radiographs, check around each bone on the radiograph looking at the cortex. Specifically, check the tarsals and the base of 5th metatarsal.
Beware of accessory ossicles - do not misdiagnose as fractures:
os trigonum (posterior to talus)
os subtibiale (distal to the tip of medial malleolus)
os subfibulare (distal to the tip of lateral malleolus)
Tibia/fibula check
-
trace around the distal tibia and fibula on both views
fractures may be accompanied by ligamentous injury and may be unstable
-
on the lateral view carefully look at the fibula
an oblique fibula fracture may be difficult to see
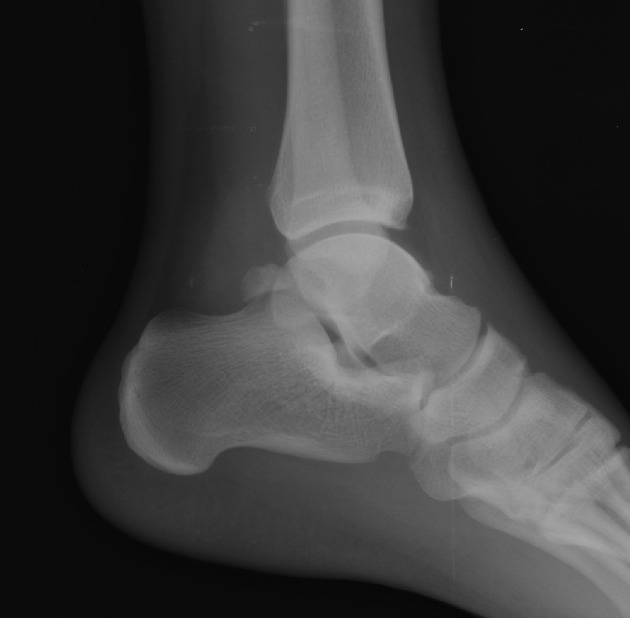
Lateral
trace the bony cortex of the lateral and medial malleoli, posterior tibia, calcaneum, and base of 5th metatarsal
-
assess Böhler angle: two tangent lines drawn across the anterior and posterior borders of the calcaneus form an angle measuring 25-40°
if <20°, think calcaneal fracture
confirm with axial view
Alignment
On the radiograph, the horizontal portion of the distal tibia parallel to the dome of the talus is the tibial plafond. Taken with the medial and lateral malleoli, it forms a rectangular socket, the ankle mortise (a.k.a. mortice 1).
Being a synovial joint, the ankle joint (between the ankle mortise and talar dome) is surrounded by a joint capsule. Like the knee joint capsule, the ankle capsule has an additional cranial extension at the syndesmosis.
Stability
The ankle is most at risk of injury when it is pronated or supinated. Pronation is relatively limited because of the shape of the medial malleolus and the deltoid ligament. This explains why only 20% of injuries occur in pronation compared to 80% when the foot is supinated.
Trace the mortise
trace around the mortise and talar dome
-
check the joint space is uniform
if one side is widened, look for a fracture
-
ensure the talar dome surface is smooth
if there is a defect or cortical irregularity, think osteochondral fracture
-
assess the interosseous ligament
1 cm proximal to the tibial plafond, the distance between the tibia and fibula should be <6 mm
if it is >6 mm, think tear or rupture of ankle ligaments and look for a fracture
Common pathology
Lateral malleolar fracture
isolated lateral malleolar fractures are common
-
the Weber classification is used to determine treatment
Weber A: below the ankle joint with intact syndesmosis
Weber B: at the level of the ankle joint
Weber C: above the ankle joint with medial malleolus fracture
Maisonneuve fracture
distal tibiofibular syndesmosis disruption
associated medial malleolar fracture, medial collateral ligament rupture, AND proximal fibular fracture
the result of traumatic external rotation
complex, unstable injury
more: Maisonneuve fracture
Pilon fracture
distal tibial fracture
compression injury usually after a fall from a height
check for associated talar or calcaneal fracture
more: pilon fracture
Calcaneal fracture
60% of all tarsal fractures; majority intra-articular
fall from height (lover’s fracture)
Böhler angle <20° indicates fracture
more: calcaneal fracture
Talar neck fracture
most common fracture of the talus
forced dorsiflexion with axial load
high risk of avascular necrosis and degenerative arthritis
more: talar neck fracture
Special paediatric fractures
Tillaux fracture: Salter-Harris type III fracture of tibia
Triplane fracture: Salter-Harris type IV fracture of tibia; most common fracture in adolescence
Don’t miss…
Osteochondral fracture
focal areas of damage to cartilage and adjacent subchondral bone
occur secondary to compressive or rotational microtrauma
commonly affects talar dome; subtle therefore frequently missed
more: osteochondral fracture











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.