
Ascending aortic aneurysms are the most common subtype of thoracic aortic aneurysms and may be true or false aneurysms.
On this page:
Epidemiology
Ascending aortic aneurysms represent 60% of thoracic aortic aneurysms.
Clinical presentation
Typically ascending aortic aneurysms are an incidental finding and the patient is asymptomatic. Rarely, the patient may present with symptoms and signs of rupture (e.g. pain, hypotension).
Pathology
Ascending aortic aneurysms are defined as a permanent dilatation of the ascending aorta ≥1.5 times the expected normal diameter or ≥5 cm in people <60 years. An ascending aortic diameter ≥4 cm is considered dilatation 7.
Aetiology
True aneurysms can result from a wide variety of conditions:
atherosclerosis (uncommon)
False aneurysms are seen in the setting of trauma, particularly deceleration injuries, as well as potentially post-thoracic aortic surgery.
Radiographic features
Plain radiograph
Ascending aortic aneurysms may manifest as a widening of the aortic or mediastinal silhouettes. The ascending aorta usually does not form part of the right cardiomediastinal margin in the first five decades. If it does, suspect dilatation or aneurysm formation.
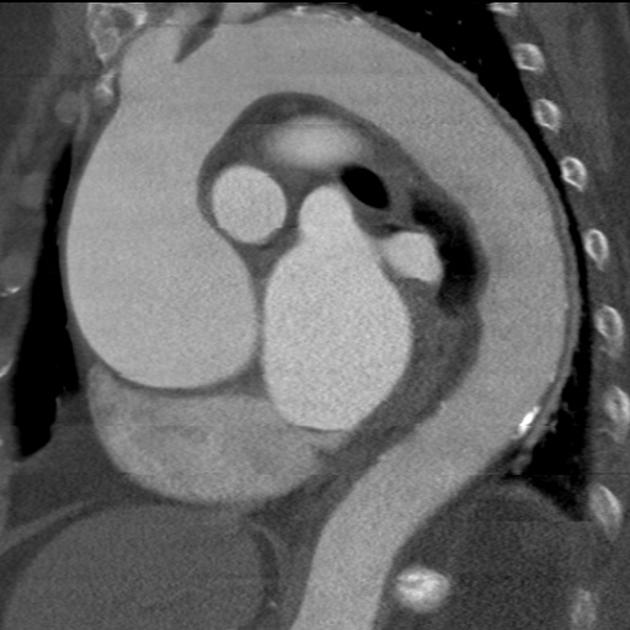
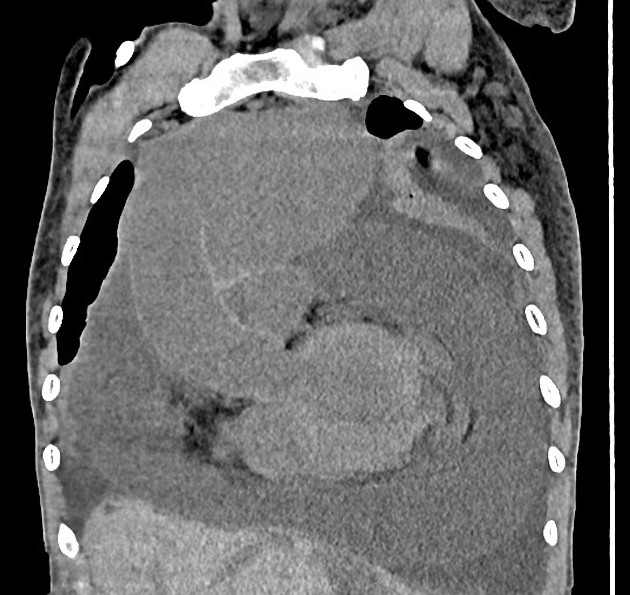
CT/MRI
ECG-gating results in superior image quality and pulsation artifacts often result in over-estimation of the ascending aortic diameter 5. Pulsation artifact is very common in non-gated CT scans, seen in up to 92% 8.
The diameter of the ascending aorta should be measured at multiple levels, making follow-up scans more accurate for comparison 4,5:
level of the aortic annulus
level of the aortic sinus
level of the sinotubular junction
mid ascending aorta
high ascending aorta (just inferior to the brachiocephalic trunk)
MRI may be preferred over CT for long-term follow-up, especially in younger patients in view of minimising radiation exposure.
Treatment and prognosis
As with other aortic aneurysms, increasing size results in an increased risk of rupture with the risk of rupture of ~7% per year in patients with an aneurysm >6.0 cm 5.
Treatment is advocated in patients with an aneurysm >5.0 cm or 5.5 cm in diameter or increasing at >0.5 cm per year. Smaller ascending aortic dilatation (>4.5 cm) is accepted in patients undergoing aortic valve replacement 4.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.