
Cardiac amyloidosis (plural: amyloidoses) is a significant source of morbidity among patients with systemic amyloidosis and is the most common cause of restrictive cardiomyopathy outside the tropics.
On this page:
Pathology
Amyloidosis represents the extracellular deposition of insoluble fibrillar proteinaceous material in various organs and tissues in a variety of clinical settings. For a general discussion of the condition please refer to amyloidosis.
Cardiac involvement is seen with most forms of amyloidosis, although it is most common and most often clinically significant with primary amyloidosis (i.e. associated with multiple myeloma or other monoclonal gammopathies).
Two main forms of amyloidosis significantly affect the heart:
AL amyloidosis: acquired disease
-
transthyretin-related (ATTR) amyloidosis: there are two types of TTR-related amyloidosis:
genetic form: variant transthyretin-related amyloidosis (ATTRv)
non-hereditary form: senile amyloidosis (ATTRwt)
Radiographic features
Ultrasound
Echocardiography
Described transthoracic echocardiography findings include
-
considered a characteristic feature of cardiac amyloidosis
characteristic granular/sparkling appearance of the left ventricular (LV) myocardium: not specific and needs to differentiate from other infiltrative diseases
-
increased LV wall thickness
results from amyloid infiltration of interstitial space and may relate to amyloid burden
-
decreased LV end-diastolic volume
leads to reduced stroke volume despite near-normal LVEF
-
typically preserved or mildly reduced LV ejection fraction
systolic dysfunction may occur in advanced disease
-
transmitral flow demonstrates a restrictive filling pattern
-
exaggerated E/A ratio (E>>A) with a truncated E wave deceleration time (DT)
a reduced amplitude A wave may suggest poor atrial function and a higher risk of thrombus formation
-
elevated E/e’ ratio suggestive of elevated left atrial pressure
-
pulmonary venous Doppler waveforms will demonstrate a diastolic filling predominance with an S/D ratio <1
amplitude of atrial reversal (AR) >35 cm/s
duration of AR exceeds mitral A wave by >20 ms
-
-
-
biatrial enlargement
atrial strain: can be significantly reduced
-
longitudinal strain (LS) in the left ventricle is impaired
impairment more pronounced at the base and mid-ventricular regions compared to the apex
specific patterns of left ventricular LS may differentiate amyloid from aortic stenosis and hypertrophic cardiomyopathy
-
reduced right ventricular systolic excursion velocity (S') as measured by tissue Doppler imaging
tricuspid annular plane systolic excursion and RV LS are early indicators of cardiac involvement in patients with systemic AL amyloidosis
reduced tricuspid annular plane systolic excursion (TAPSE) despite normal RV end-diastolic dimension
-
dynamic left ventricular outflow tract obstruction
distinguish from hypertrophic obstructive cardiomyopathy (HOCM)
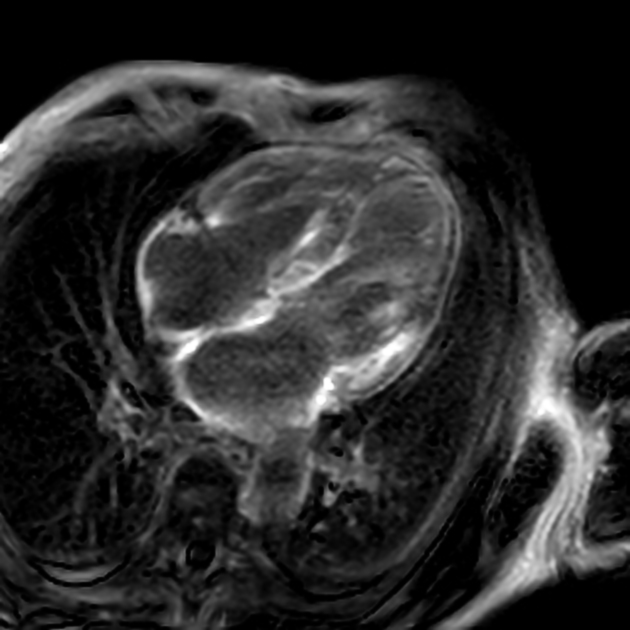
MRI
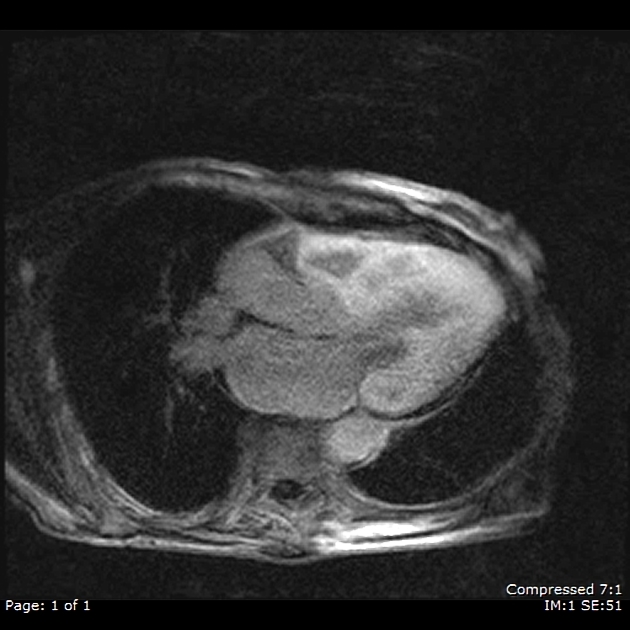
MRI is the modality of choice for evaluating cardiac amyloidosis. Features include:
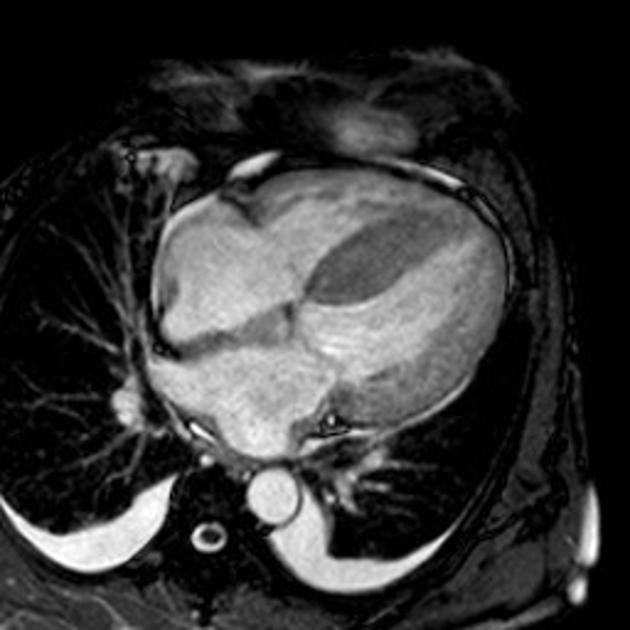
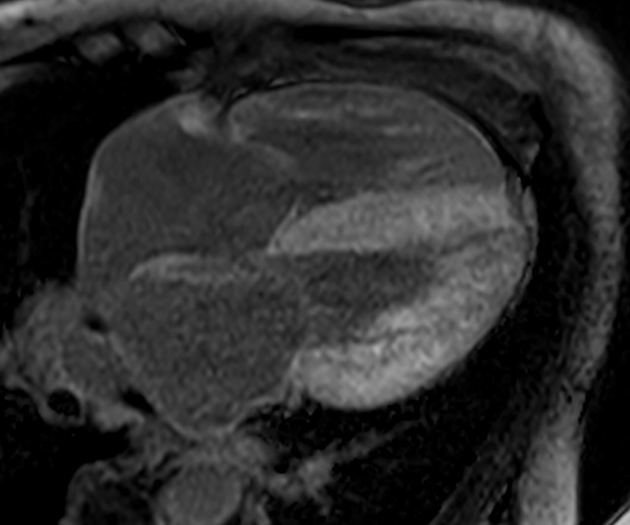
diffuse left ventricular wall thickening (usually, multiple chambers are involved); can be associated with thickening of both atrial walls in which case, a thickening of >6 mm of the inter-atrial septum or posterior right atrial wall is specific to amyloidosis 10
-
biventricular diastolic dysfunction with normal systolic function and ejection fraction
subsequently (later in the course of the disease) may show systolic biventricular dysfunction with a decreased ejection fraction
restriction of diastolic filling
disproportionate atrial enlargement
pericardial and pleural effusions
-
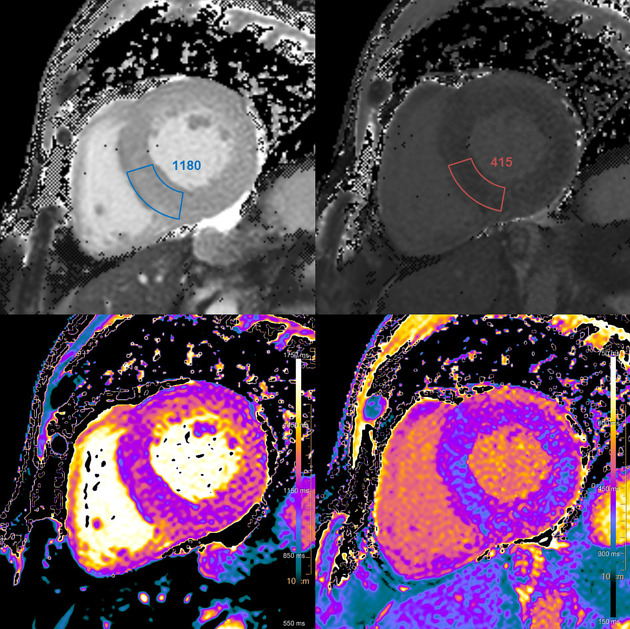
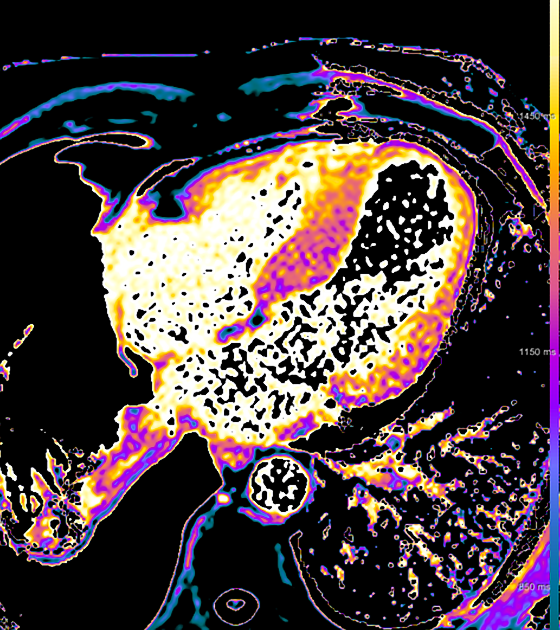
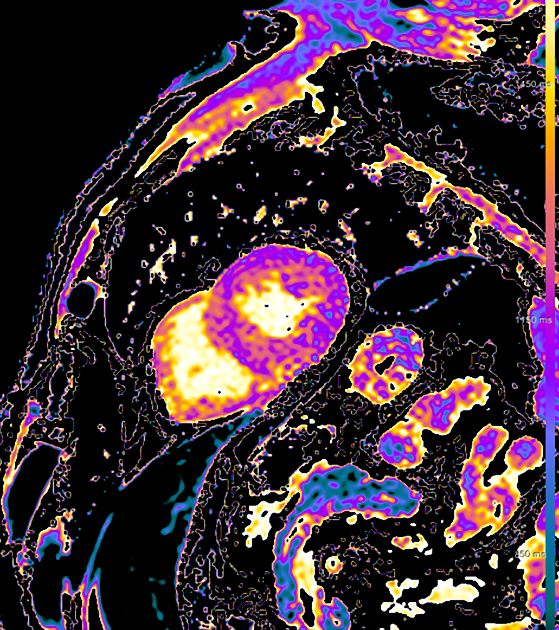
T1 mapping:
native T1 is prolonged even more in AL-amyloidosis than in ATTR-amyloidosis 13-16
extracellular volume is increased especially in ATTR-amyloidosis, for which it is a prognostic factor 15,16
-
T2 mapping:
elevated T2 is associated with a worse prognosis in AL-amyloidosis 17
-
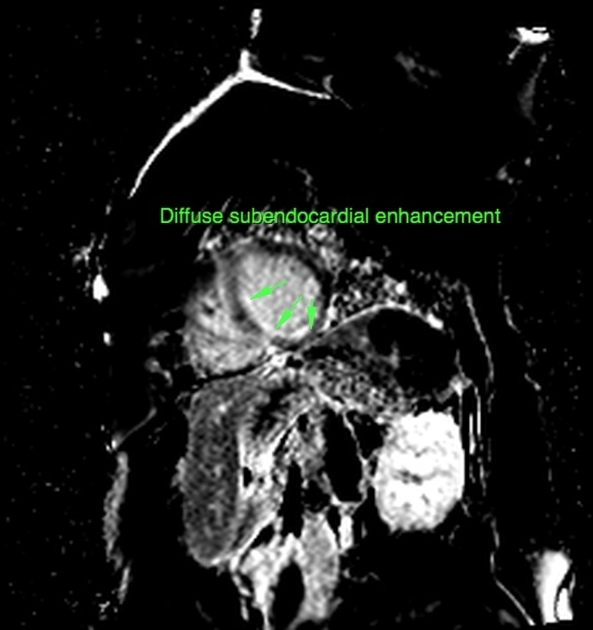
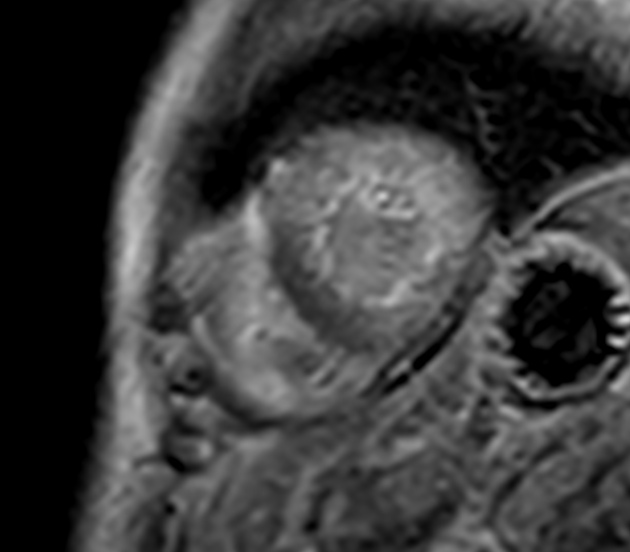
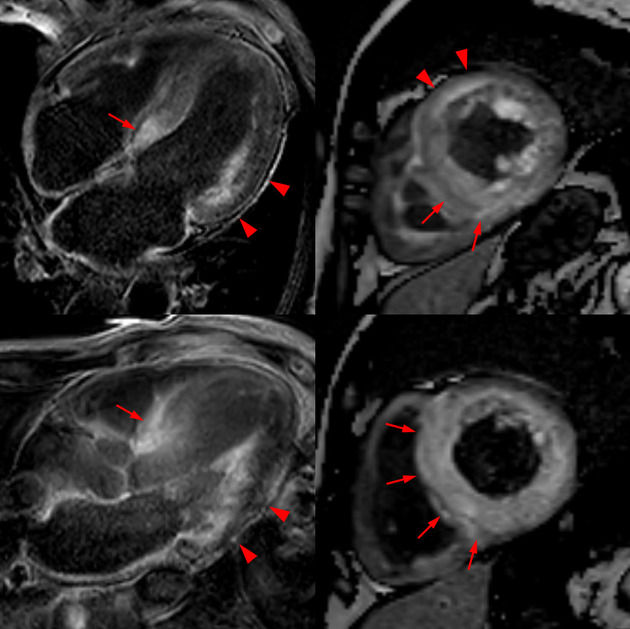
late gadolinium enhancement (LGE)
diffuse sub-endocardial heterogeneous increased signal on contrast-enhanced inversion recovery T1-weighted images (a characteristic feature) 11
transmural enhancement may be more prevalent in patients with ATTR compared to patients with AL 6
TI scout sequence: may have some diagnostic utility for the presence of myocardial amyloidosis (in terms of type I, II and III nulling patterns) 24
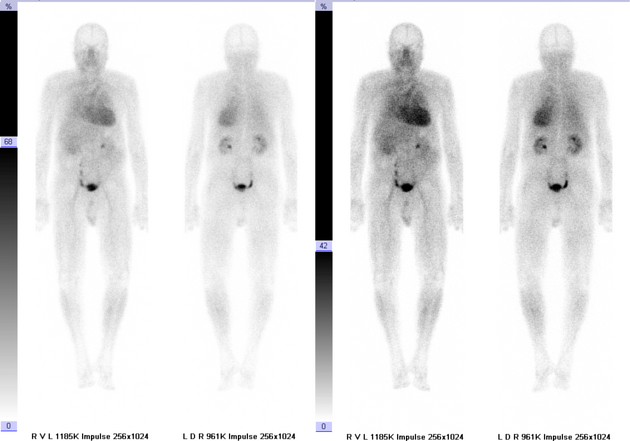
Nuclear Medicine
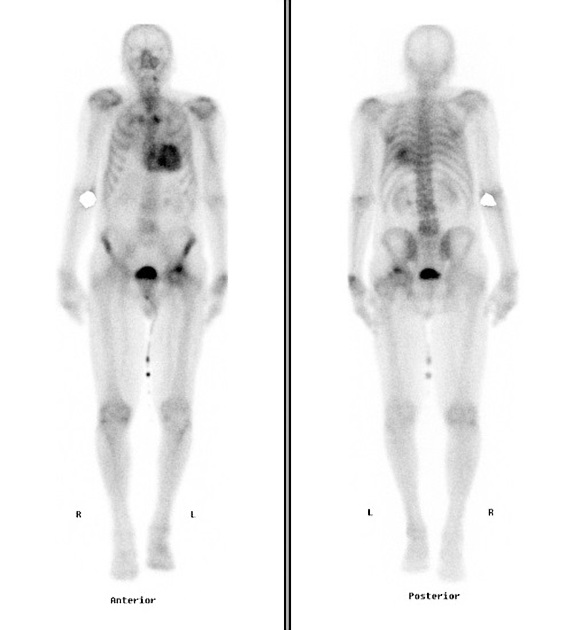
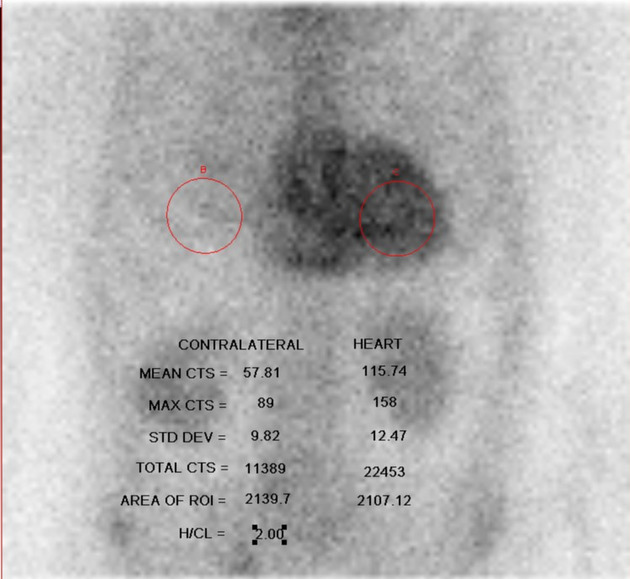
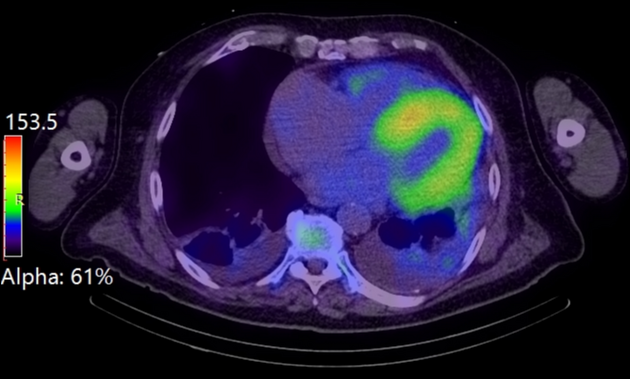
Tc-99m-DPD, Tc-99m-HMDP (hydroxy methylene diphosphonate) and Tc-99m-PYP (pyrophosphate) 22 have been shown to have high sensitivity and specificity for the diagnosis of transthyretin cardiac amyloidosis (ATTR) 19,20.
Planar +/- SPECT-CT scintigraphy is performed one hour post tracer administration. Images are assessed for the presence of abnormally increased uptake in the myocardium to indicate the presence of ATTR cardiac amyloidosis. Cardiac uptake is evaluated visually and can be scored using the Perugini scale, which compares tracer uptake in the ribs to uptake in the myocardium (if present) 18,21. A grade 2 or 3 pattern of myocardial uptake is strongly suggestive of ATTR amyloidosis, with variable scan uptake encountered in AL amyloidosis23. Delayed three-hour imaging can be performed if there is abnormal biodistribution of tracer (i.e. increased generalized soft tissue uptake) at the one-hour time point.
Differential diagnosis
Cardiac amyloidosis needs to be distinguished from other forms of restrictive cardiomyopathy, including:


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.