
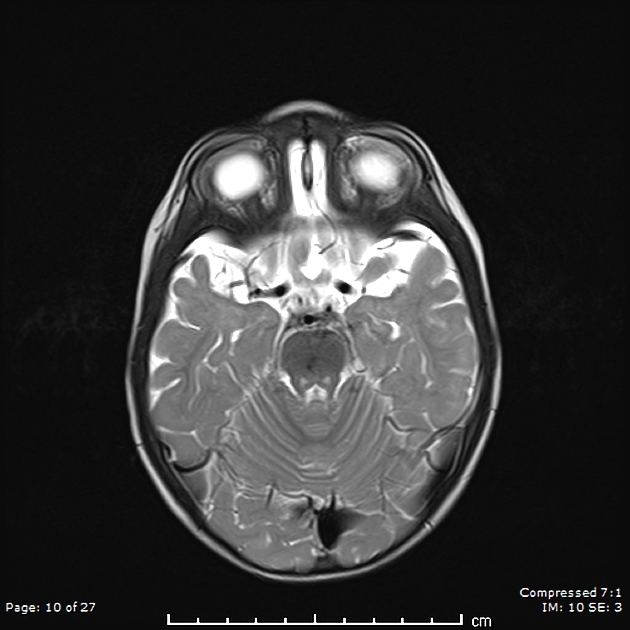
High T2 signal of the central tegmental tract, which connects the red nucleus and inferior olivary nucleus, is an uncommon finding typically encountered in early childhood.
The central tegmental tract refers mainly to the extrapyramidal tracts connecting between the red nucleus and the inferior olivary nucleus. This tract is one of the earliest regions in which myelination begins (9 months after conception) 3. Symmetrical central tegmental tract hyperintensities on T2-weighted images are an uncommon finding 2.
On this page:
Epidemiology
The symmetrical central tegmental tract hyperintensity occurs more frequently during the early childhood between 1 and 5 years of age 2,3. It is encountered in a variety of settings including 2,5:
epilepsy
metabolic disorders
Occasionally it is found in children with no clinical neurological finding 2,3.
Pathology
The aetiology is unclear and numerous theories for the pathogenesis have been suggested, including intramyelination oedema, gliosis or secondary degeneration of the cerebral white matter 1. Some authors suggest that the majority of imaging findings simply represent a physiological maturation-related process 3.
One study suggests that high T2 signal of the central tegmental tract may be linked to two distinct pathophysiological processes 7. The first process is likely transient, marked by axonal changes accompanied by diffusion restriction and increased FLAIR signal intensity 7. In contrast, the second process involves irreversible myelin degeneration, characterised by the resolution of diffusion restriction and the emergence of T2/FLAIR mismatch 7.
Radiographic features
MRI
T2: symmetrical hyperintensities in the central tegmental tracts
DWI/ADC: may show restricted diffusion
FLAIR: increased signal in transient cases; T2/FLAIR mismatch in chronic cases 7
Treatment and prognosis
The meaning of this finding, its clinical correlation with various neurologic deficits and prognosis remains unclear, and in some instances it is reversible 3,4.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.