
Cervical spine injuries can involve the cervical vertebral column, intervertebral discs and cervical spine ligaments, and/or cervical spinal cord. The cervical spine accounts for ~50% of all spinal injuries.
On this page:
Epidemiology
5-10% of patients with blunt trauma have a cervical spine injury 1.
Pathology
Patients can have a combination of injuries including:
- atlanto-occipital dissociation
- occipital condyle fracture
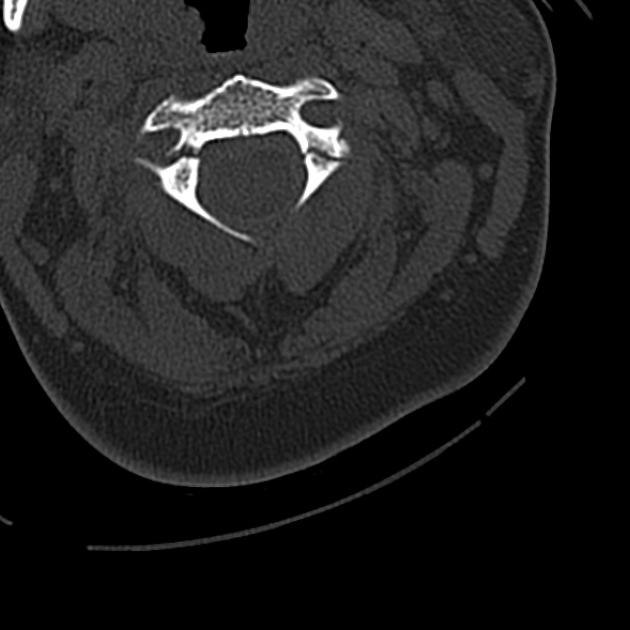
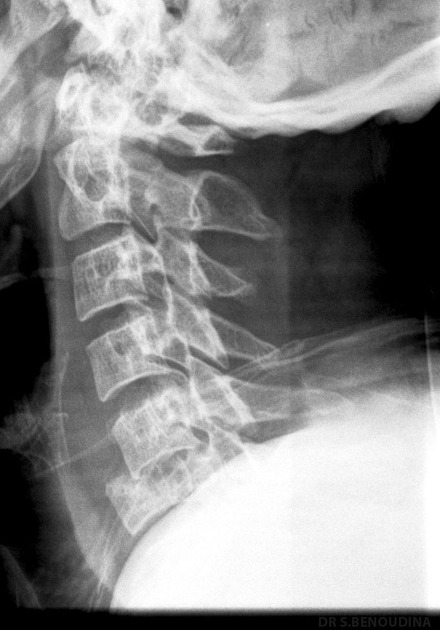
- cervical spine fractures
-
discoligamentous injury
- anterior subluxation (posterior ligamentous complex rupture)
- facet joint dislocation
- spinal epidural haematoma
- spinal cord injury
- vertebral artery dissection
Aetiology
- blunt trauma: motor vehicle accident (40%), falls, sports injuries
- penetrating trauma: gun shot injuries, stabbing
Associations
- closed head injury: patients with GCS <8 at highest risk 3
Radiographic features
CT and MRI both have roles to play. CT is used to assess patients who are obtunded, at high-risk, or those unable to be cleared by clinical criteria (e.g. NEXUS criteria, Canadian C-spine rule).
The majority of patients are imaged while being immobilised in a cervical spine collar. If the CT is reported as negative, the collar is typically removed (cervical spine collar clearance). A select few patients nevertheless require further assessment with MRI.
MRI is used to assess for discoligamentous injury but has a controversial role in patients who are obtunded and a normal CT with some advocating it as unnecessary due to the CT's high negative predictive value for unstable cervical spine injuries 1.
Please see the individual articles listed above for further details in imaging findings.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.