
Intracranial tuberculous granulomas, also known as CNS tuberculomas, are common in endemic areas and may occur either in isolation or along with tuberculous meningitis.
On this page:
Epidemiology
The epidemiology of patients with tuberculomas is the same as that of other CNS manifestations of tuberculosis (TB) (see CNS tuberculosis).
Pathology
A tuberculoma is distinct from a tuberculous abscess in that it demonstrates evidence of granulomatous reaction and caseous necrosis histologically. In contrast, abscesses do not display a granulomatous reaction and their centres are filled with pus 5,6. Not all tuberculomas, however, have a solid granulomatous core and some may undergo liquefaction 4. Tuberculous organisms may not necessarily be identified in tuberculomas, whereas they are necessary to make the diagnosis of tuberculous abscess 6.
Radiographic features
CT
On CT, tuberculomas may appear as a round or lobulated nodule with moderate to marked oedema. Either solid or ring enhancement is typical post-contrast. A central focus of calcification with a ring of peripheral enhancement (the "target sign") is described but is not specific to tuberculosis 7. When calcification is present (the minority of cases) it tends to be larger than that calcification seen in neurocysticercosis.
MRI
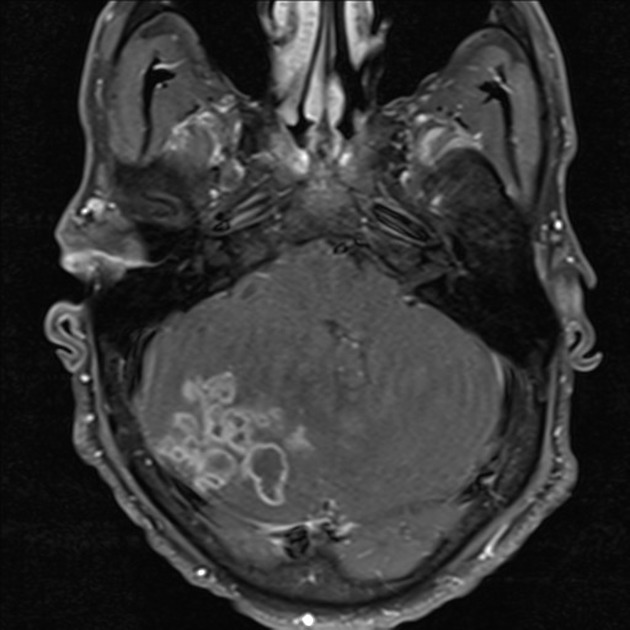
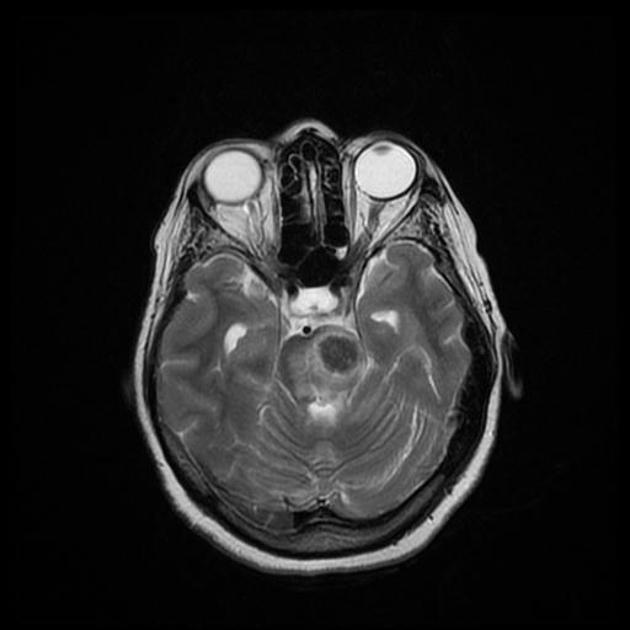
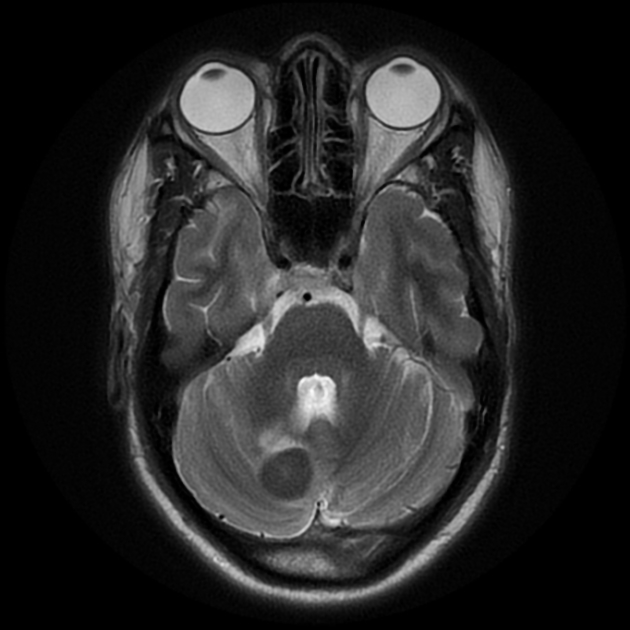
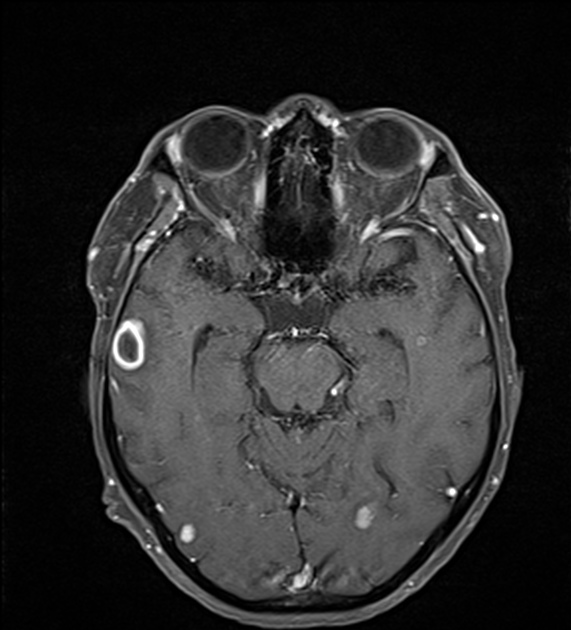
MRI is the modality of choice in assessing potential tuberculomas. Although the appearance can be classical and highly suggestive of the diagnosis (central low T2 signal, surrounding enhancement and oedema) it does, however, vary with the stage of disease 1,3,8,9. In some instances, when liquefactive necrosis occurs central, the imaging appearances are essentially indistinguishable from a tuberculous abscess, which in turn is similar to pyogenic cerebral abscesses 4.
Non-caseating granuloma
- T1: iso- to- hypointense
- T2: hyperintense
- FLAIR: no suppression
- DWI/ADC: no restricted diffusion
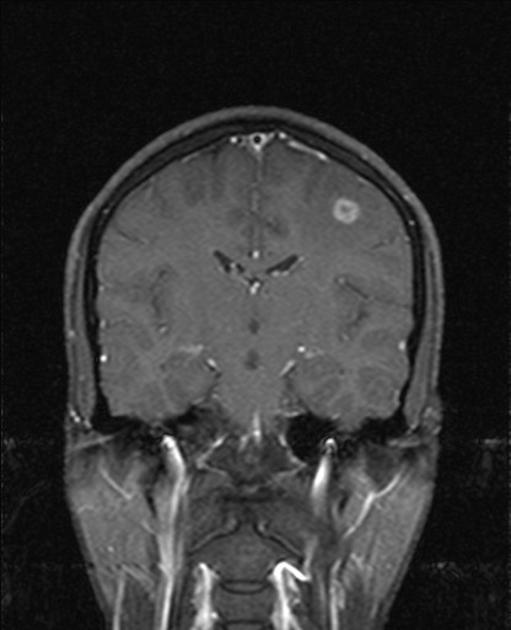
- T1 C+ (Gd): homogeneous enhancement
Caseating granuloma
- T1: iso- to- hypointense with hyperintense rim
-
T2:
- hypointense representing gliosis and abundant monocyte infiltration 1
- surrounded by vasogenic oedema
- FLAIR: no suppression
- DWI/ADC: no restricted diffusion
- T1 C+ (Gd): homogeneous or ring-enhancement
-
MR spectroscopy
- decrease in NAA/Cr
- slight decrease in NAA/Cho
- lipid-lactate peaks are usually elevated (86%) 2
Caseating granuloma with central liquefaction
- T1: iso- to- hypointense with hyperintense rim
-
T2:
- hypointense rim with central hyperintensity
- surrounded by vasogenic oedema
- FLAIR: partial suppression
- DWI/ADC: variable diffusion restriction
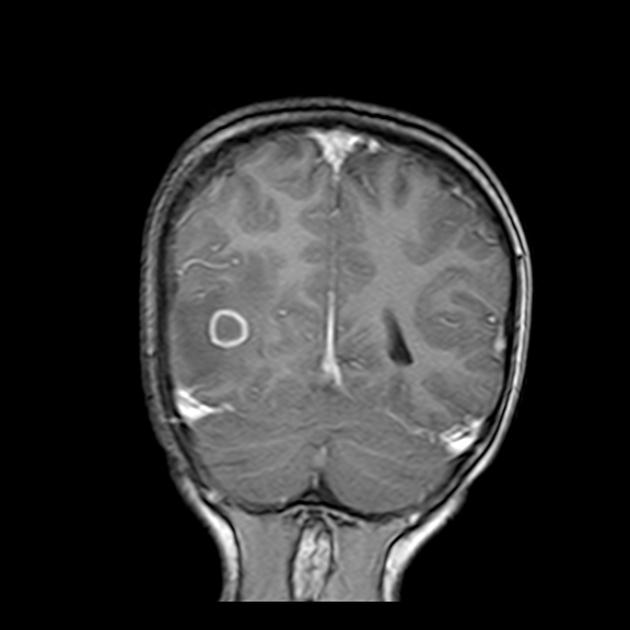
- T1 C+ (Gd): ring enhancement
Calcified granuloma
- T1: iso- to- hypointense
- T2: hypointense
- FLAIR: no suppression
- DWI/ADC: no restriction
- T1 C+ (Gd): no enhancement
Differential diagnosis
The differential of tuberculomas is primarily the differential of ring-enhancing lesions and includes:
- other infection
- neurosarcoidosis
- cerebral metastases
- CNS lymphoma
Central isointensity or hypointensity compared to grey matter seen centrally on T2 is helpful, as it is not seen in most other causes 1.












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.