
Cowden syndrome, also known as multiple hamartoma syndrome, is characterised by multiple hamartomas throughout the body and increased risk of several cancers.
On this page:
Terminology
Type 2 segmental Cowden syndrome is the association of Cowden syndrome with a Cowden naevus when it is considered a type of epidermal naevus syndrome.
Clinical presentation
The disease is characterised by 7:
-
mucocutaneous lesions: present in >90% of cases
acral (palmoplantar) keratoses
intellectual disability
-
thyroid abnormalities
gastrointestinal hamartomatous polyps (small and large bowel)
lipomas, including testicular lipomatosis 6
In addition to benign tumour formation, Cowden syndrome carries a recognised increased risk of multiple malignancies 1,7:
breast cancer: develops in 30-50% of those with the syndrome
thyroid cancer: develops in 5% of those with the syndrome, usually follicular
endometrial cancer: develops in 5-10% of those with the syndrome
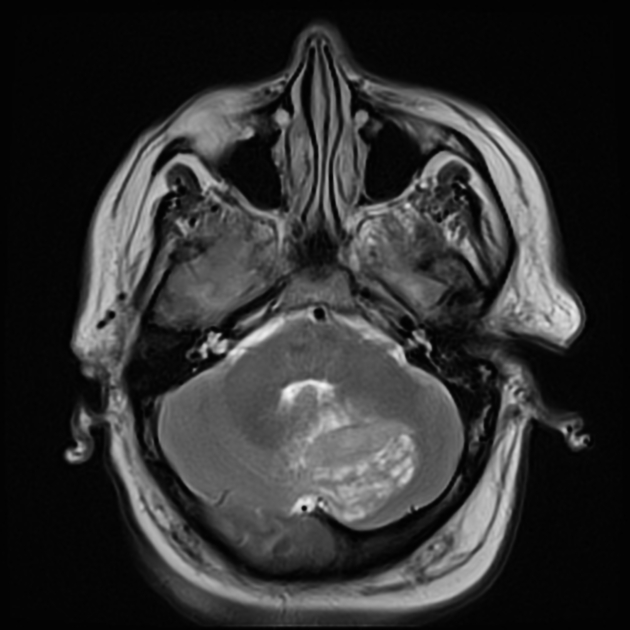
CNS: dysplastic cerebellar gangliocytoma, occurs when in association with Lhermitte-Duclos disease
possible increased risk of renal cell carcinoma, colorectal carcinoma, and melanoma
Pathology
Genetics
It carries an autosomal dominant inheritance with variable (but high) penetrance 7. A gene locus for the disease has been identified on chromosome 10q22-23, a mutation of the PTEN gene 7.
Thus, Cowden syndrome is part of a group of disease known as PTEN-related diseases, which also includes 3,7:
History and etymology
First described in 1963 by K M Lloyd and M Dennis with the surname of their first patient: Cowden 2.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.