
Fetal pleural effusions (FPE) refer to an accumulation of pleural fluid in utero. It can refer to either a fetal chylothorax or a fetal hydrothorax.
On this page:
Images:
Pathology
A fetal pleural effusion can occur as part of hydrops fetalis, in association with other anomalies without hydrops or in isolation - primary pleural effusion/primary fetal hydrothorax (PFHT).
Causes
Any cause of hydrops fetalis is a potential aetiological factor in a fetal pleural effusion.
Associations
In addition to hydrops fetalis, pleural effusion can be associated with numerous other underlying anomalies:
congenital cardiac anomalies: ~ 5% of non hydropic pleural effusions 1
-
underlying congenital lung anomalies
-
chromosomal anomalies 1,3 (can be present in ~ 50% with an additional sonographic abnormality and ~ 12% without an additional sonographic abnormality 9)
Down syndrome: ~ 20% (range 5-33%) of non hydropic pleural effusions 1,7
Turner syndrome: especially with a 1st trimester pleural effusion
polydactyly: ~ 1% of non hydropic pleural effusions 1
Radiographic features
Ultrasound
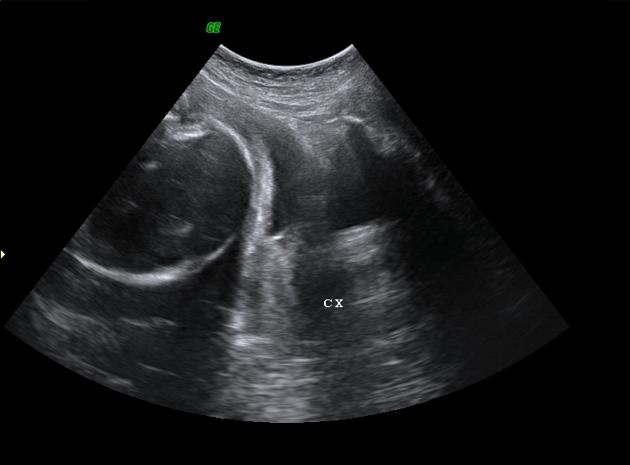
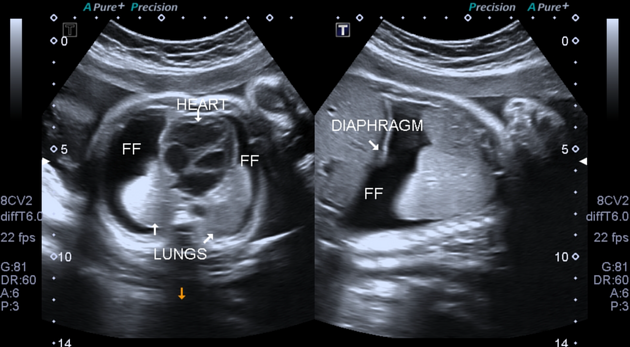
Classically seen as anechoic fluid surrounding one or both the lungs (which are echogenic) - batwing appearance.
Ancillary sonographic features include:
may show other features of hydrops if it occurs in association
there maybe presence of polyhydramnios (if severe)
Treatment and prognosis
The clinical course is variable and dependent on aetiology. The presence of a pleural effusion early in pregnancy (i.e. first trimester) is often associated with a poor fetal outcome 5.
Management options are also dependent on other underlying factors:
thoracocentesis and drainage of the effusion: fluid can however reaccumulate within 24-48 hours
insertion of pleural-amniotic shunts




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.