
IgG4-related hypophysitis is a rare cause of inflammation of the pituitary gland and an uncommon manifestation of the systemic IgG4-related disease (IgG4-RD).
On this page:
Epidemiology
Although IgG4-RD tends to present in middle-aged and elderly men, the gender ratio is more balanced in patients with IgG4-related hypophysitis and other head and neck manifestations of IgG4-RD 1.
Clinical presentation
Clinical features depend on the part of the pituitary gland involved 1-3:
-
adenohypophysitis (anterior pituitary involvement):
hypopituitarism or individual endocrine hormone deficiencies (e.g. hypothyroidism, hypogonadism)
mass effects on adjacent structures (e.g. optic chiasm)
infundibuloneurohypophysitis (posterior pituitary involvement): diabetes insipidus
panhypophysitis (both anterior and posterior pituitary involvement): all of the above clinical features
Pathology
IgG4-related hypophysitis is characterised by chronic inflammation of the pituitary gland with histology revealing lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells 1,2. This classic histological finding differentiates it from the histological appearances of other aetiologies of hypophysitis, those being:
lymphocytic hypophysitis: lacks plasma cells and presents in a young female demographic 1,2
granulomatous hypophysitis: has multinucleated giant cells that form true granulomas, is secondary to diseases such as neurosarcoidosis, and also tends to present in a young female demographic 1,2
xanthomatous hypophysitis: has foamy histiocytes (xanthoma cells) and macrophages 1,2,6
necrotising hypophysitis: extremely rare and has necrosis with only scattered pituitary tissue remaining 1,2,7
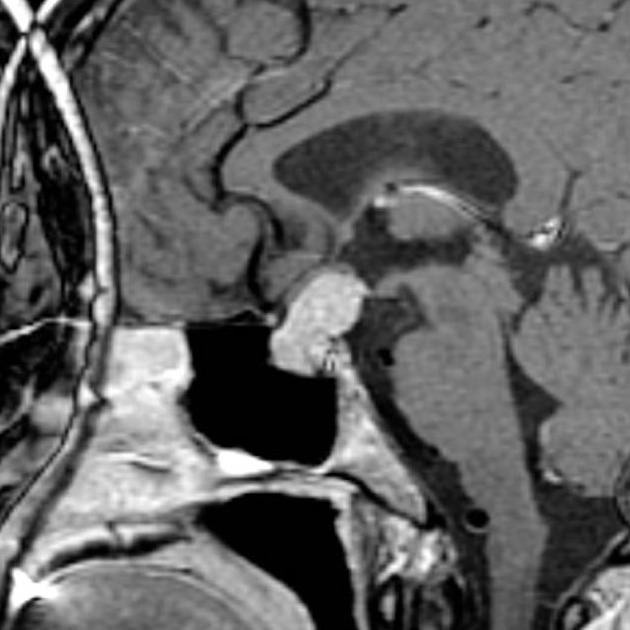
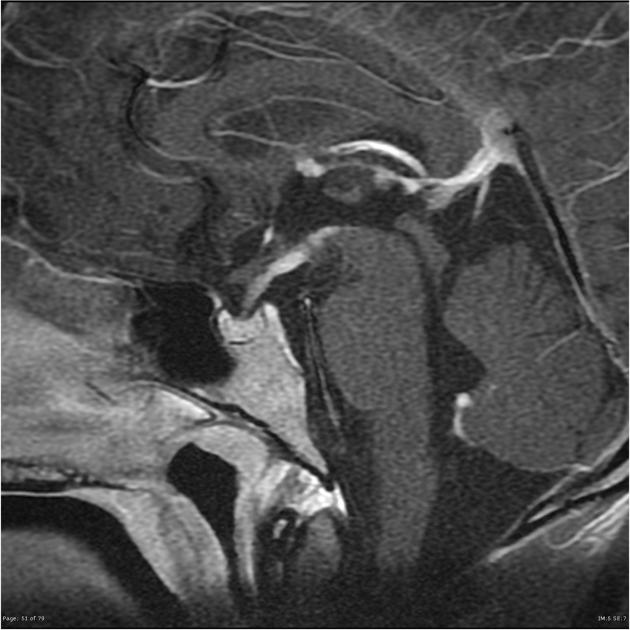
Radiographic features
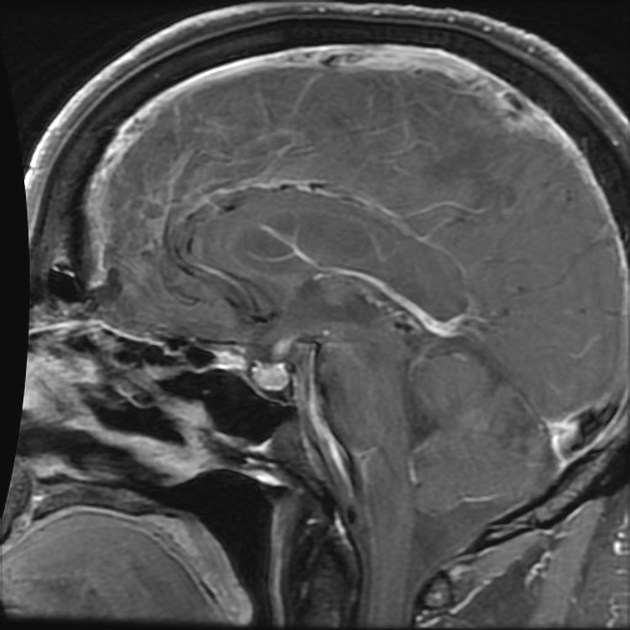
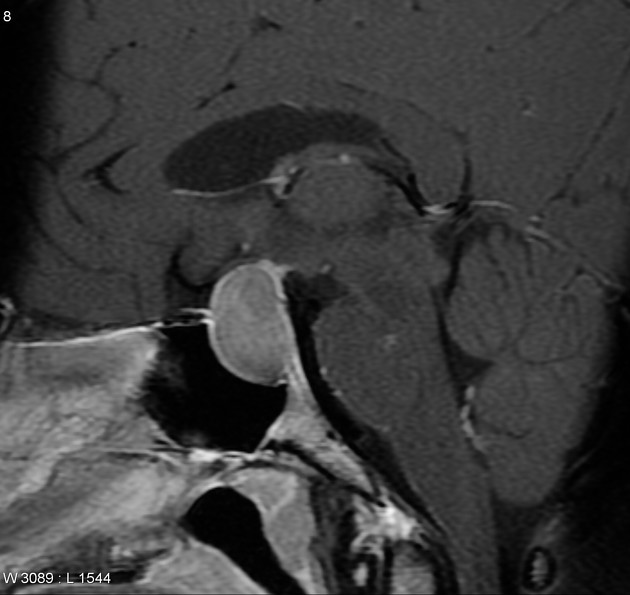
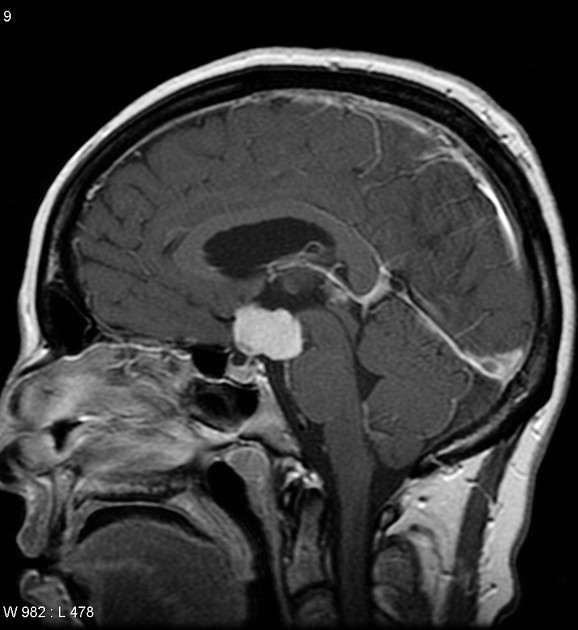
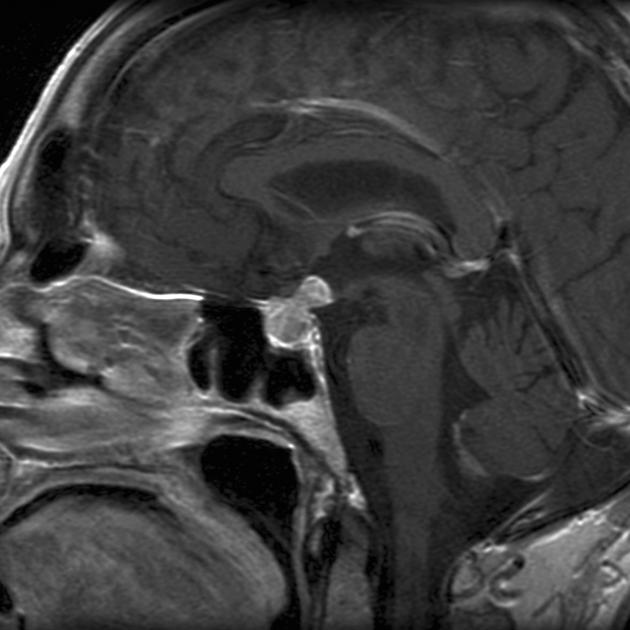
Although this is a very rare entity, common radiographic findings that have been reported include non-specific enlargement of the pituitary gland with or without infundibulum enlargement that is visible on both CT and MRI 1,4,5. Post-contrast T1-weighted MR images may further reveal enhancement 1,4,5.
Other associated head and neck manifestations of IgG4-RD, such as IgG4-related hypertrophic pachymeningitis, may also be seen 1,4,5.
Treatment and prognosis
Based on case series-level evidence, good response is seen to corticosteroids such as prednisolone or hydrocortisone 1,2. Treatment of endocrine hormone deficiencies (e.g. giving desmopressin for diabetes insipidus) is also prudent 1,2.
Differential diagnosis
The differential diagnosis is primarily that of other pituitary region masses. Considerations include:




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.