
Intravenous urography (IVU) is a radiographic study of the renal parenchyma, pelvicalyceal system, ureters and urinary bladder using intravenous contrast medium. This exam has been largely replaced by CT urography.
On this page:
Terminology
The term "urography" refers to evaluation of the entire urinary tract, ie. kidneys, pelvicalyceal systems, ureters and bladder. Intravenous pyelography (IVP) or excretory urography (EU) are commonly used as alternative but less accurate terms. Some reserve the term "pyelography" to refer to retrograde opacification of the collecting system.
Indications
IVU is rarely performed if CT is available. However if a CT IVU demonstrates delayed excretion due to obstruction, a delayed radiograph following CT IVU can identify the site of obstruction.
IVU can provide important information:
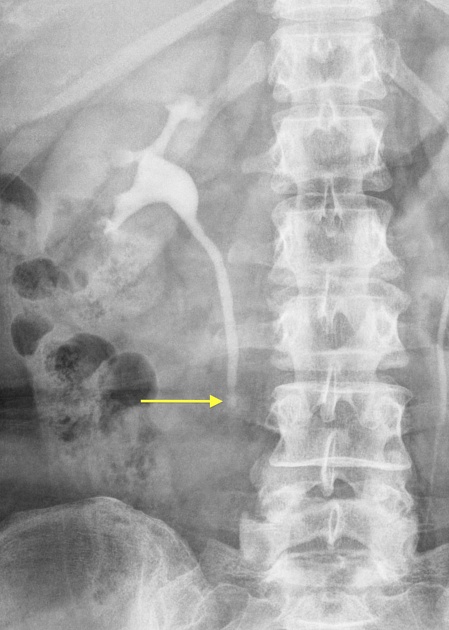
ureteric obstruction: severity, site and cause e.g. urolithiasis
synchronous or metachronous upper tract tumour: detailed evaluation of pelvicalyceal and ureteral morphology in patients with bladder transitional cell carcinoma (TCC)
papillary necrosis
anatomical variants such as horseshoe kidney
the course of the ureters
renal function
Patient preparation
fasting for 5 hours prior to the examination is preferred; laxatives to reduce faecal loading do not improve image quality 4
check eGFR
check for allergies and contrast medium reactions and obtain written informed consent according to hospital guidelines
emergency medications and equipment must be available to treat clinically significant contrast medium reactions
Technique
Exposures in the 65-75 kV range optimise radiographic contrast, mA of 600-1000 and exposure time < 0.1 second.
There are various IVU techniques 4. 18 or 19G gauge IV access is required for bolus injection of a water-soluble iodinated contrast agent; nonionic contrast medium has a better safety profile. A dose up to 1.5 ml/kg body weight is well tolerated.
For suspected ureteric obstruction the following radiographs will suffice:
control AP radiograph of the kidneys, ureters and bladder to show calculi which can be obscured by contrast medium
3 minute post injection AP radiograph of the kidneys to show contrast medium beginning to appear in the pelvicalyceal systems. Unilateral absent excretion indicates obstruction. Cortical and medullary nephrogram is normally well seen at 3 minutes but attenuation may be reduced on the obstructed side
10 minute full-length AP radiograph, optional obliques
full-length post-micturition radiograph to confirm ureteric obstruction and delineate the lower ureter which can be obscured by contrast medium in the bladder
if the obstruction is severe and the ureter is insufficiently opacified, perform delayed full-length radiographs at 1 hour +/- 24 hours
High-grade obstruction can significantly delay excretion. The nephrogram on the obstructed side will be delayed, and will persist and increase in attenuation. If the site of obstruction is not delineated at 1 hour, then a 24-hour delayed radiograph is indicated.
Contrast medium is heavier than urine and this property can be used to advantage. An erect full-length radiograph will demonstrate a full ureter to the point of obstruction. If the patient cannot stand, lie them prone to demonstrate the mid ureter and then supine to show the distal ureter.
The technique for synchronous or metachronous upper tract urothelial tumours includes detailed views of the pelvicalyceal systems and ureters.
5 minute AP radiograph of the kidneys then apply a lower abdominal compression band to distend the upper tracts
AP and both oblique radiographs of the kidneys at 10 minutes
full length AP radiograph and both obliques on compression release
prone views are optional to show the mid ureters
multiple images help overcome the problem of non-visualisation of ureteric segments due to normal peristalsis
AP full-length post void view
Compression is contraindicated in:
large abdominal mass
abdominal surgery (post operative)










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.