
Isolated greater trochanteric fractures most commonly result from forceful muscle contraction of a fixed limb, which usually occurs in those who are young and physically active.
On this page:
Epidemiology
Isolated trochanteric fractures are more common in young, active males, usually between the ages of 14 and 25 ref. 85% of mild trochanteric avulsion fractures occur in patients <20 years ref. In the elderly, trochanteric fractures are usually due to direct trauma, such as a fall ref.
Clinical presentation
Patients will present with pain, especially the lateral hip and on abduction and extension, exacerbated on palpation ref.
Pathology
Greater trochanteric fractures are a subtype of trochanteric fractures and can be isolated or non-isolated ref.
Mechanism
Most commonly due to:
avulsion type fracture: forced muscle contraction of the hip abductors and external rotators, usually due to physical activity
direct trauma of the greater trochanter, e.g. due to a fall onto the lateral hip
Radiograph features
Plain radiograph
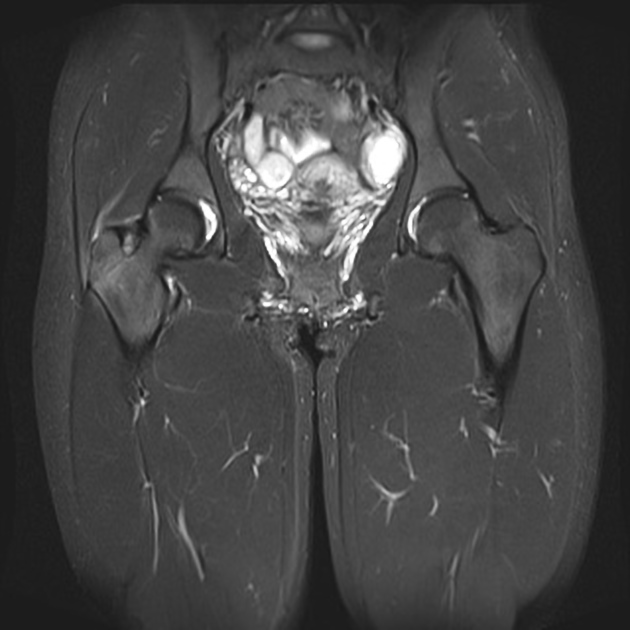
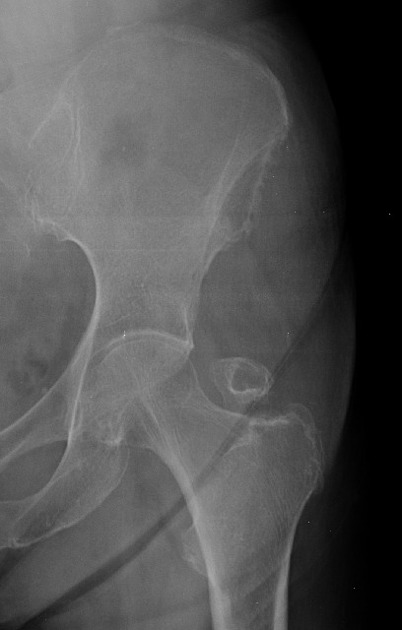
Anterior-posterior (AP) and lateral or oblique radiographs are usually sufficient for diagnosis. They generally show an apophyseal avulsion fracture of the greater trochanter.
Treatment and prognosis
Most trochanteric fractures are self-limiting and can be treated without surgical intervention if the displacement is less than 1 cm. However, the patient must not bear weight on the affected leg for up to a month. Many patients may take up to 3 months to return to normal physical activity.
Complications of isolate trochanteric fractures are quite rare, usually manifesting as a slight loss of abduction force.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.