
Neonatal bowel obstruction is the most common neonatal abdominal surgical emergency 1. It is generally divided into high and low obstruction according to the level of the transition point, since imaging appearances, underlying pathology, treatment, and prognosis differ.
It is divided into:
high bowel obstruction - proximal to the ileum
low bowel obstruction - involving the ileum or colon
On this page:
Epidemiology
It is estimated to occur in about 0.05% of all live births 2.
Clinical presentation
The clinical presentation is not specific and depends on the location of the obstruction. But usually, neonates will present with:
abdominal distension and tenderness
bilious vomiting
constipation
feed intolerance
bile-stained vomit/aspirates
respiratory distress with acidosis
sepsis, blood-stained stools, or diarrhoea in case of necrotising enterocolitis
failure to pass meconium in the first days
Pathology
Aetiology
High obstruction
ileal atresia or stenosis
Low obstruction
Small bowel obstruction
Large bowel obstruction
colonic atresia or stenosis
anal atresia and anorectal malformations
Radiographic features
Plain radiograph
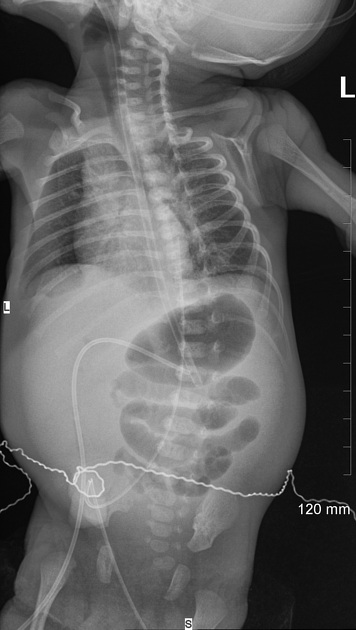
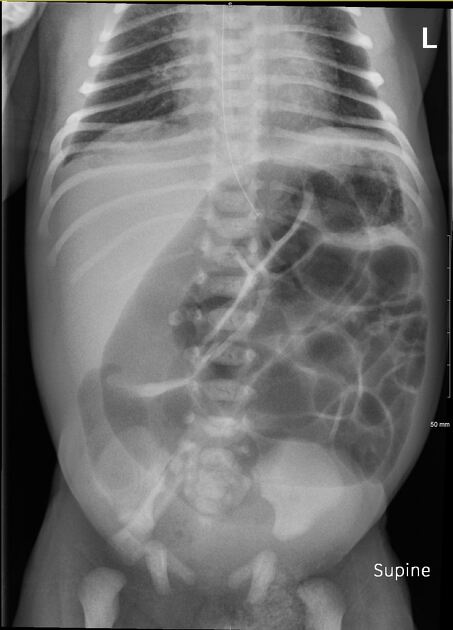
Abdominal radiographs are the first imaging modality in neonatal acute abdomens. The features vary widely depending on the level of the obstruction, and generally demonstrate:
dilated bowel loops: bowel diameter greater than the interpedicular width of L1 3
-
number of dilated loops
high obstruction <3 dilated loops
low obstruction >3 dilated loops
absence of rectal gas: can be confirmed only if the radiograph is performed >24 hours after birth
air-fluid levels: due to ineffective peristalsis
-
small bowel or colon involvement
if there is no gas in the rectum, AP abdominal radiographs are unreliable to differentiate the colon from small bowel, since haustra are hard to identify in neonates 4
to differentiate small and large bowel in neonates, a colon enema may be performed
-
intramural bowel gas: suggestive of necrotising enterocolitis
granular faeces should not be seen in the neonatal bowel (exclusive milk diet); if seen, it is indicative of pneumatosis intestinalis
Fluoroscopy
Contrast enema is usually performed, to locate the level of obstruction. The features depend on the cause of the obstruction.
Ultrasound
Ultrasound is the second line imaging modality for assessing acute abdomens in neonates. It may show:
dilated bowel loop
ineffective peristalsis
prominence of the valvulae conniventes
Findings suggestive of bowel ischaemia:
extraluminal free fluid
loss of peristalsis
bowel wall thickening with effacement of mural architecture
Treatment and prognosis
The treatment depends on the aetiology of the obstruction.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.